Why Does a Man Have Bilateral Nodular Densities on Chest Radiograph
A 28-year old man comes in who recently arrived in southern California from South America and suddenly developed a "cold." His symptoms included productive cough, shortness of breath, chest pain, fever, weakness and malaise. He also reported unexplained weight loss. Sputum and blood specimens were obtained for acid-fast smear examination and culture. A single posterior-anterior chest radiograph was obtained as part of his initial evaluation.
HISTORY
A 28-year old man comes in who recently arrived in southern California from South America and suddenly developed a “cold.” His symptoms included productive cough, shortness of breath, chest pain, fever (often accompied by chills), , weakness and malaise. He also reported unexplained weight loss. Sputum and blood specimens were obtained for acid-fast smear examination and culture. A single posterior-anterior (PA) chest radiograph was obtained as part of his initial evaluation.
PHYSICAL EXAMINATION
On admission, he presented with mild tachypnea and tachycardia; palpable enlarged cervical lymph nodes, mild swelling in the axilla, a fever of 103.6, and a blood pressure of 150/80, with a pulse of 92.
Radiographic Findings
The PA chest radiograph displayed diffuse fine granular nodular densities in a miliary distribution throughout the right and left lungs (Figure1). A low dense margination of the pericardium separates the heart from the surrounding lungs. An enlarged view of the PA chest (Figure 2) clearly defines miliary densities. This zone of decreased density (increased metallic silver) reflects the effect of the heart beating against the edematous (wet) lung. A definite pleural effusion is not demonstrated. The remaining cardiomediastinal structures are not unusual.
Diagnosis
The differential diagnosis should include miliary tuberculosis (TB), San Joaquin Valley fever (Cocciomycosis), and disseminated fungal infection (which is more common in immune compromised hosts) such as Pneumocystis carinii. In this case, the diagnosis of miliary TB was confirmed by the identification of Mycobacterium tuberculosis in the acid-fast sputum smear.
Discussion
Miliary tuberculosis represents with widespread hematogenous dissemination of tubercle bacilli. In children, it is often caused by a recent primary infection and in adults, it can be the result of recent infection or reactivation of old disseminated disease. (1)
Most patients have fever, night sweats, anorexia, weakness, and weight loss. (1) This patient’s country of origin provides a clue to the diagnosis. Of the tuberculosis cases diagnosed in foreign born residents of the United States in 2014, China, India, Mexico, the Philippines and Vietnam are responsible for more than half of the foreign born tuberculosis patients in the United States (2).
Though the numbers have been declining globally, there were 9 million new tuberculosis cases and nearly 1.5 million fatalities in 2013, according to the World Health Organization.
There were just 9,412 new cases of active tuberculosis in the United States in 2014, a 2.2% point decline from the previous year. Of those, more than half appeared in Asians and Hispanics, the vast majority of whom were born abroad. (2)
REFERENCES
1. RAVIGLIONE MC, OBRIEN RJ. TUBERCULOSIS. IN FAUCI AS, Braunwald E. Isselbacher KJ, et al, eds. Harrision Principles of internal medicine. 14th ed. New York, NY. Mc Graw-Hill, 1998:1004-1014.
2. Centers for Disease Control and Preventive Reported tuberculosis in the United States, US Department of Health and Human Services, CDC, 2014. www.cdc.gov/tb.
3. Diagnostic Standards and classification of Tuberculosis in Adults and Children. This official statement of the American Thoracic Society and the Centers for Disease Control and Prevention was adopted by the ATS board of directors, July 1999. This statement was endorsed by the council of Infectious Disease Society of America, September 1999. Am J. Respir Crit Care Med 2000, 161:1376-1395
TAKE HOME MESSAGE
The knowledge of a patient’s history, landmark anatomy and the pathophysiology that accompany a particular disease is important in making an accurate diagnosis from plain radiographs. Our patient presented with the signs and symptoms of a disease that is very characteristic of tuberculosis and coccidiomycosis.
Even if a person has symptoms of tuberculosis, it is often difficult to diagnose. A chest X-ray should be obtained to determine if changes of the disease are present. If the radiograph is negative, a follow-up chest x-ray should be obtained. A qualified radiologist should interpret the chest radiograph.
FIGURES

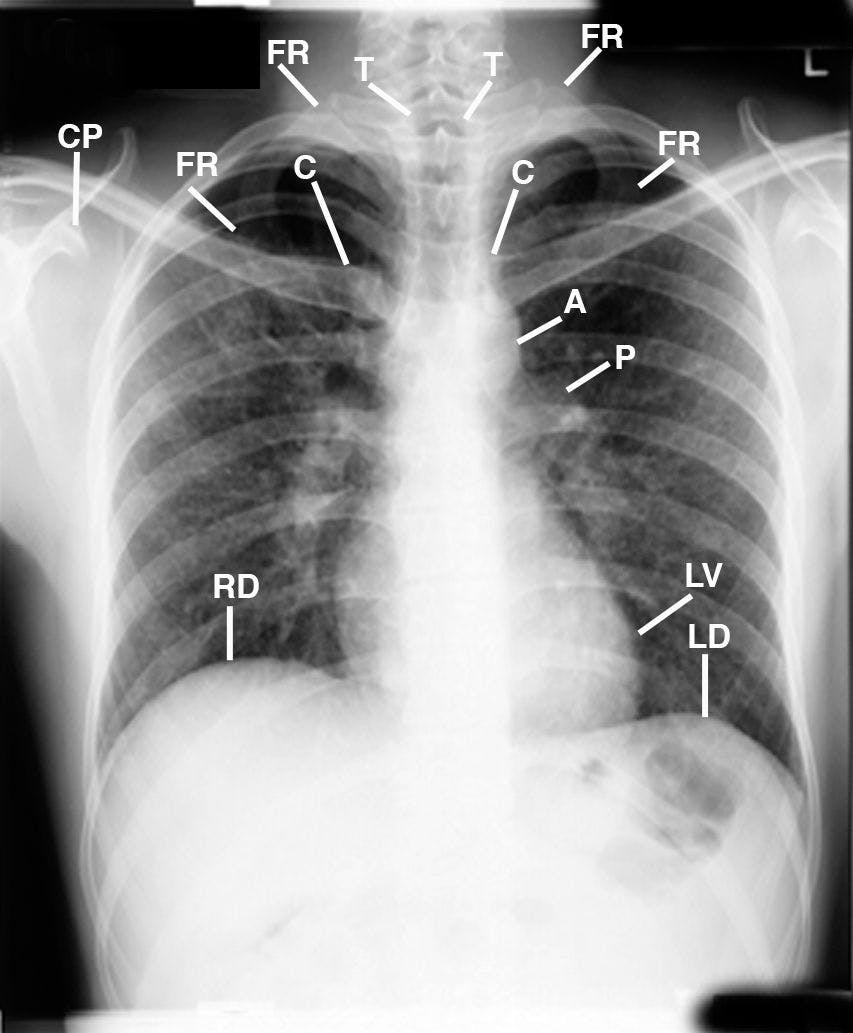

Figure 1 is a Posterior Anterior (PA) chest radiograph that displays the patient leaning right accentuating mild right concave cervicothoracic spine scoliosis C3-T12 (not labeled); drooping forward right shoulder as compared to the elevated left shoulder; anterior rotated heads of the clavicles low over the 5th posterior ribs, right lower than left; enlarged hilar lymph nodes (not labeled); multiple small nodular densities throughout both lungs; increased lucency marginating the pericardium (not labeled) reflecting the beating heart pumping away the adjacent edematous lung. Aorta (A), Head of the clavicle (C), Coracoid process (CP), First rib (FR), Left and Right diaphragm (LD, RD), Left Ventricle (LV), Pulmonary artery (P), Trachea (T).

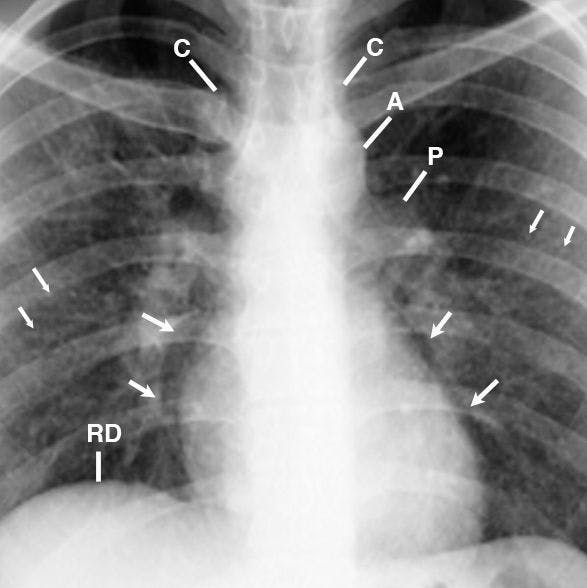

FIGURE 2 is a cone down enlargement of FIGURE 1 that displays fullness of the hila reflecting enlarged lymph nodes (not labeled); bilateral lucent margination of the pericardium as above described on Figure 1 (4 large arrows); and the multiple small nodular densities throughout both lungs (4 small arrows). Aorta (A), Head of the clavicle (C), Right hemidiaphragm (RD), Pulmonary artery (P).



3. FIGURE 3 is a inverted image of the left side of the thorax that gives a different perspective of the lucent margination of the heart as above described in Figure 2. Observe the grayish display of the small nodules in the left lung (small arrows).














