Blood Pressure Monitoring and Substance Use Considerations With Esketamine
Geoffrey Grammer, MD, offers guidance on navigating challenges such as elevated blood pressure and substance misuse and abuse regarding the use of esketamine.



Transcript
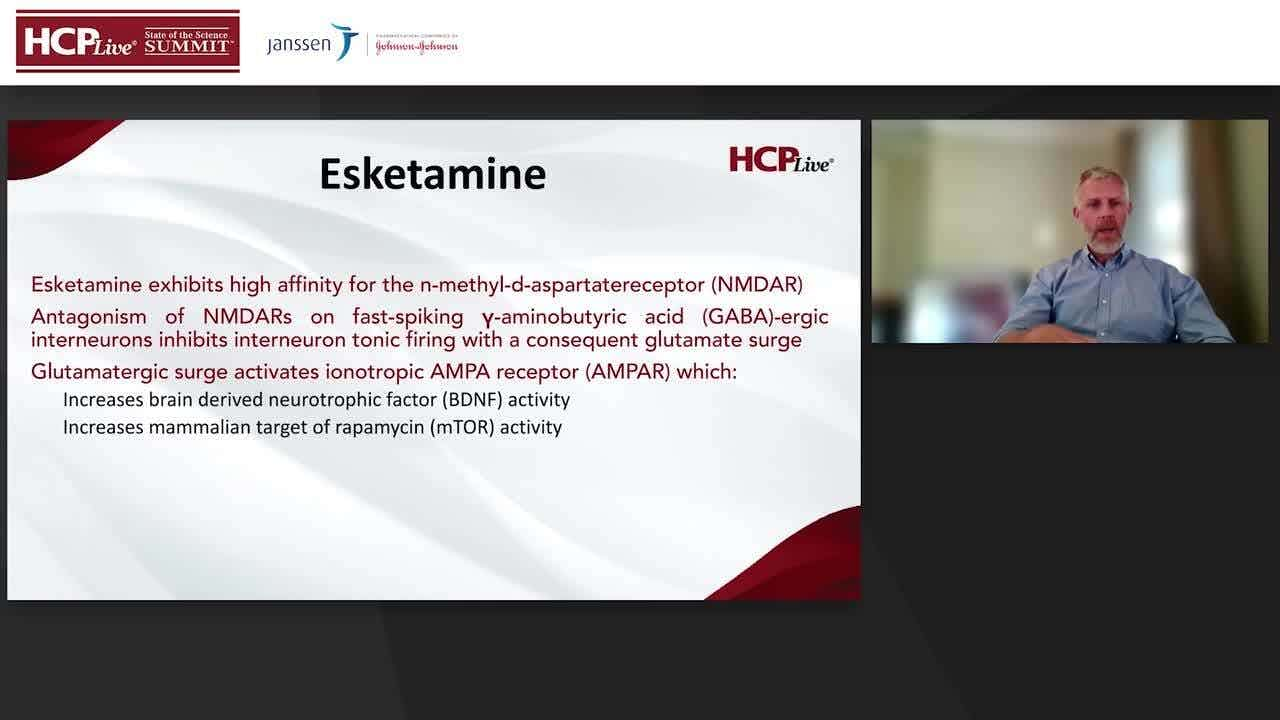
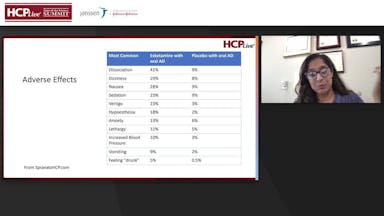
Geoffrey Grammer, MD: I found this first statistic to be intriguing. 8 to 19% of nasal esketamine treated patients experienced a greater than 40mmHg increase in systolic blood pressure and a greater than 25mm in mercury in diastolic blood pressure in the first one and a half hours after administration. So, if you think about that, that's pretty important, because if someone comes in and their blood pressure is like 160 over say 90 and you take them to a systolic for example, of 200, that makes that a much more anxious visit. Right? And where you have to control their blood pressure. So just be mindful that the increase in blood pressure can be pretty substantial. The other thing to consider is that that increase in blood pressure can occur even if they haven't had that increase beforehand. So don't get necessarily reassured if they tolerated earlier blood pressures with Spravato and say, "well, the last time it was only ten point systolic or whatever. And then, you know, this time they should be fine if their blood pressure for that particular day is elevated because they didn't take their meds" or what have you. And then, anyone who has any medical condition where you're considering an increase in blood pressure where that could destabilize the medical condition you want to think hard and long about whether to give that person's Spravato. I'll give you an example of someone of something that is not necessarily within that package insert, aortic stenosis, which is very dependent upon after load. If you suddenly change their after load, that could destabilize their underlying, you know, cardiac output and potential heart failure if that's associated with aortic stenosis. \
Let's talk about substance use disorders. And this one is a difficult one. Individuals with a history of drug abuse or dependance may be at greater risk of abusing or misusing nasal esketamine. Frequently used (more than weekly) large doses of ketamine, like in the population for illicit use, can be associated with withdrawal symptoms, cravings, fatigue, poor appetite and anxiety. While there were no reports of drug seeking behavior in the phase three clinical trials, just be aware that the intoxication or the mental status changes that occur with ketamine can actually trigger people's cravings for certain substances. Also, make sure that you're doing this in a supervised setting. The reason why we're not seeing addiction to nasal esketamine is because it's been given under that supervised, tightly controlled setting. So [as for] the abuse potential, they took 34 patients who had a history of recreational drug use. They gave them a single dose of nasal ketamine and IV ketamine. They measured the drug liking at the moment. And drug take drug again, measurement. And these are two measurements to say, you know, how much did you like it and how much do you feel like you might want to take it again? And basically, both IV ketamine and nasal esketamine had elevated scores on those two metrics compared to those who got placebo. So, it can be triggering for some patients with a past history of addiction. So, what are the signs that someone might be misusing substances or in some cases nasal less ketamine? Attempted diversion. So, people are saying, "hey, you know, twice a week isn't enough for my induction, can I do three times a week?" Or "hey, I want to do maintenance at twice a week, is that okay?" When they're deviating from the FDA guidelines, that ought to be a cue to ask them about what they actually think the benefit of ketamine might be, because it's not the intoxication from the nasal esketamine or the mental status changes that leads to the therapeutic effect. It's the mechanism that Dr Chopra and Dr Sauve talked about and the sort of dissociation and sedation that comes with nasal less ketamine is more of a side effect. Also, if they're asking for higher doses, like, "hey, 84 milligrams is not enough. Can I get, you know, a fourth vial?" That ought to kind of flag that maybe something else is going on here. Symptoms of drug craving or withdrawal, particularly if they're using illicit ketamine or if they're trying to get other forms of ketamine, like the lozenges and IV, which may not necessarily be reported. Those can often be misinterpreted as depressive symptoms so you start increasing frequency of treatment again to try to recapture remission, when in fact, you may be dealing with a substance misuse. Then anyone who develops interstitial cystitis, that wasn't observed in the trial, so be very suspicious on whether or not they're getting ketamine from another source.
Blood pressure monitoring is really critical. Know what the levels are, know where your thresholds are, know how to access higher levels of care. And really one guideline to follow is just be very careful in treating anyone with a blood pressure higher than 140 over 90. And that metric is actually in the package insert. While you can always use your clinical judgment, I would be very cautious in treating anyone over that level to start with. It doesn't take a lot to get control of the blood pressure. A lot of times these patients aren't even on medications or they're not taking it. Get control, bring them in, it's safe, and then you're good. Substance use history requires additional considerations for patients and additional monitoring. Just be aware of that because while nasal less ketamine itself may be safe when given in the manner that has been recommended, when it's given in the context of the entire patient condition, you may find it may be causing other problems.
Transcript was AI-generated and edited for clarity.