Emerging Agents in Psychedelic Therapy for Treatment Resistant Depression
William M. Sauve, MD, reviews the landscape of delivery mechanisms for ketamine agents, including intravenous, sublingual, and intramuscular.



Transcript
William M. Sauve, MD [In terms of] emerging agents, I would like to start with ketamine, and ketamine can mean 3 different things in broad categories. Number one is intravenous (IV) ketamine; that has been around for quite some time. Then we have "other" ketamine, and that includes sublingual, intramuscular (IM). [Then], there's a few other things. You can go to a compound pharmacy with a ketamine prescription, and they will do whatever you want with it, whether it makes sense or not. But sublingual and IM are probably 2 that are maybe the most studied. Then there's esketamine, which Dr Harvey alluded to, and we'll get into a little bit more detail about that.
A couple quick things to know [about] IV ketamine: Good old racemic ketamine was FDA approved for anesthesia in 1966. It's been studied in the context of depression since approximately 2000, and that would be studies at [the] National Institutes of Health (NIMH) and at some universities. It's maybe a little bit more complicated than this, but the IV form has been traditionally favored secondary to bioavailability. And the general rule [of] oral ketamine is maybe 10% bioavailable, no more than 20%, depending on who you ask. So [the] ketamine pill is, for the most part, going to get destroyed in your liver; and then there's some other forms that we'll get into a little bit more later. But IV is by definition 100% bioavailable. You can dose it by weight, and it makes it a little bit easier to use. You can see the attraction to that when you're in the study environment. I did find this particular citation from 2023 getting into ketamine esketamine. From this particular paper, there were a couple of take-home points. Number one, IV ketamine for depression and many other indications [is being widely used]. I'm saying that as diplomatically as possible. In other words, all the indications are being used widely with very little standardization. So, ketamine is ketamine. It's been around a long time. It's relatively ubiquitous. It's a schedule 3 substance, it is not that hard to get. It is being used in rather uncontrolled fashion all over the country. Sometimes, depending on where you go, you're going to get what you get.
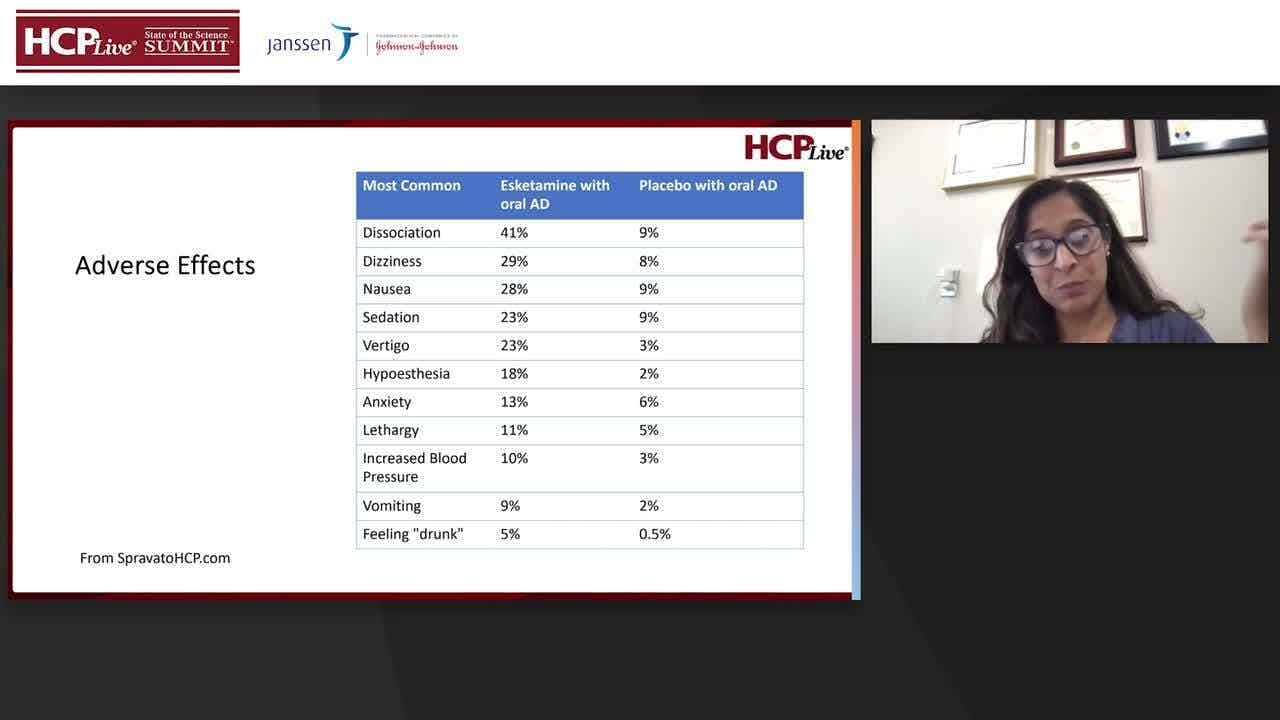
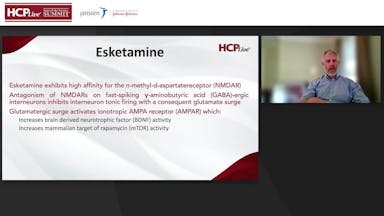
Esketamine, as Dr Harvey alluded to, is the S-enantiomer, that's the left-handed an enantiomer molecule of ketamine. It was FDA cleared for treatment resistant depression in 2019. [The] intranasal form of ketamine is approximately 30 to 50% bioavailable. So, it's not 100% like an IV, but 30 to 50% bioavailable can get you enough of a dose to be clinically useful. That's shown in the studies that led to FDA approval. It's maybe slightly unpredictable, but predictable enough that it's been working well in the clinic. Esketamine exhibits a high affinity for the n-methyl-d-aspartate receptor (NMDAR) receptor. The beauty of that is that we're on the NMDA receptor, we are not necessarily on the serotonin, the dopamine and serotonin receptor, which is kind of been the thing for the past 60 years. So, this is NMDAR, an antagonism of NMDAR on fast-spiking gamma-aminobutyric acid (GABA)-ergic interneurons inhibits interneuron tonic firing with a consequent glutamate surge. Glutamatergic surge is activating ionic tropic AMPA (AMPAR), which is going to increase brain derived neurotrophic factor (BDNF) activity, which is like the Miracle-Gro for your brain; and I think most people think that that's a good thing. It also increases mammalian target of rapamycin activity, which is something all the cool kids have been talking about for quite a few years.
The whole idea here is growth and connections and growth and flexibility in the brain. Some lower activity targets also include activation of new kappa and the delta opioid receptors. So, it does that action there [with a] caveat. There was a lot of talk about the metabolites of ketamine activating opiate receptors. There was at least one study where ketamine was combined with naltrexone and then the ketamine didn't work; that was seen as the mechanism of action. Then someone did another study where we combined ketamine with naltrexone, and it totally work. So, for now, the literature is equivocal, 50/50 over whether or not the opiate receptor is necessarily that critical to the mechanism. But ketamine and esketamine do have action ultimately on that receptor. There is also some weak inhibition of serotonin, dopamine, [and] norepinephrine, transporters. So, it's not the main thing, because we're still focused on NMDAR, but it is part of it. And it is an agonist at D2 and it's an antagonist of 5-HT3. This is exciting because it has been suggested that MDMA assisted therapy might be approved within the next year. So, keep your eye on that and we'll see what happens.
For now, MDMA is one of the compounds that was given breakthrough status from the FDA. This is very exciting and looking for an opportunity to use it therapeutically. It was actually first synthesized in 1912 and patented in 1914. This is a chemical that's been around for a very long time. And the interest in clinical use actually goes all the way back to the 30s and 40s. But now in some recent years, as the psychedelics have had a bit of a resurgence, the data is piling up and this might be something that we'll be able to use officially, clinically very soon. This drug also has serotonin reuptake inhibition as well as dopamine and neurotransmitter and to a lesser degree, and possibly increased oxytocin. Systematic review and meta-analysis suggest twice as many subjects with PTSD no longer met criteria for the disorder with MDMA assisted therapy versus placebo, and that's just kind of the latest in 2023. So, the data for this has been piling up and it is getting very exciting. Next on the list is psilocybin. Psilocybin also was given breakthrough status by the FDA. Several private players are working to come up with something that will be FDA approvable, and that might be two, maybe 3 years away from the latest I'm hearing. So, we're looking at that very carefully too. Psilocybin assisted therapy is highly encouraging for multiple applications, but definitely for TRD. A recent study suggested not only efficacy for depression, but the important thing here is that benefit was sustained up to a year. So, it isn't just that it's thought to work, but it's thought that maybe one session, two sessions, have actually resulted in changes that persisted for 12 months. And you can see that quote from the 2022 trial that said exactly that.
Transcript was AI-generated and edited for clarity.