Patient Education Key to Gout Treatment Adherence
Effective treatment for gout management does exist, but without patient compliance, gout exacerbations continue to be common. Here: strategies to get buy-in from the patient.


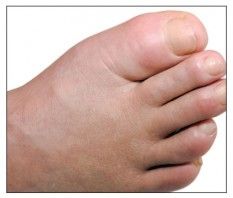
Gouty arthropathy. Photo courtesy Ayeh M. Abeles, MD and Michael H. Pillinger, MD
One of the biggest challenges rheumatologists face in treating patients with gout is convincing them to fully participate in their own care and to maintain their treatment regimen. Effective treatment for gout management does exist, but without patient compliance, gout exacerbations continue to be common.
The authors of a new review pointed out that barriers to ULT adherence may be caused by several issues-- from misunderstanding the role of ULT to medication costs. “Adhering to these treatment regimens is often challenging for gout patients,” the authors wrote. “Patients can be confused regarding the different treatment approaches with ‘as needed’ dosing for acute gout and long-term therapy for chronic gout.”
The number of patients with gout is rising. A 2013 study from the UK found a 63.9% increase in prevalence and 29.6% increase in incidence of gout between 1997 and 2012. On average, the standardized prevalence increased 4.2% per year, while incidence rose 1.5%. But despite this increase, patient adherence to ULT remained suboptimal.1
According to the study, in 2012, 48.48% percent of patients were specifically treated for gout or treated with ULT (allopurinol, febuxostat, benzbromarone, probenecid, or sulfinpyrazone). Among them:
- Only 37.63% actually received ULT.
- 18.6% received ULT within 6â months of diagnosis.
- 27.3% of incident gout patients received ULT within 12â months of diagnosis.
Although the percentage of adherent patients was still low, it did improve somewhat, from 28.28% in 1997 to 39.66% in 2012.
The review authors described a study that used a pharmacist-based program to help increase patient treatment adherence. Published in 2014, this study looked at 100 patients, aged 21 to 94 years old, with chronic or recurrent gout. A trained clinical pharmacist and rheumatologist worked with each patient by phone. The patients also received educational and dietary materials, and they followed a standard gout treatment protocol with the goal of achieving and maintaining a serum uric acid level of 6â mg/dL or less. Of the 95 evaluable patients, 78 met and kept their goals.2
A similar study published in 2013 used specialist nurses to monitor patients by phone or in person, encouraging them with their lifestyle changes, and providing education about gout and the importance of medication adherence. Of the 106 patients who participated in the study, nine out of ten successfully reached target levels.3
The authors of the review acknowledged that while there have been some improvements in gout therapy adherence through patient monitoring, nonadherence to gout treatment may also be related to ethnic differences, patient age, and financial constraints. “Given the burden of gout on the population and its associated impact on patients, more investigation is needed into novel approaches to address barriers to optimal medication management to a target sUA level as well as incorporation of lifestyle changes,” they concluded.
References:
1. Kuo CF et al. Rising burden of gout in the UK but continuing suboptimal management: a nation-wide population study. Ann Rheum Dis. 2014;0:1–7.
2. Goldfien RD et al. Effectiveness of a pharmacist-based gout care management programme in a large integrated health plan: results from a pilot study.BMJ Open. 2014;4:e003627.
3. Rees F, Jenkins W, Doherty M. Patients with gout adhere to curative treatment if informed appropriately: proof-of-concept observational study. Ann Rheum Dis. 2013;72:826–830.














