A Russian Bride With Hip Pain
A 48-year-old woman presented to the orthopedic clinic with dull, persisted pain in the sacroiliac area that was impervious to NSAIDs. She denied knowledge of any injury or other possible explanation.
The Case:



A 48-year-old woman presented with a 2-month history of right-sided hip pain.
Located in the sacroiliac area, the pain was dull and constant. It persisted despite use of NSAIDs.
She denied knowledge of any hip injury or other inciting event.
Other Findings:The dermatology clinic had evaluated pruritis.
Physical examination in the gynecology clinic revealed uterine enlargement. Results of pelvic ultrasonography were pending at the time she was seen in orthopedics.Laboratory Results:-- elevated thyroid-stimulating hormone (TSH)
-- normal thyroxine
-- hemoglobin: 11.1 g/dL (normal: 11 to 15 g/dL)
-- hematocrit: 32.3% (normal: 34% to 46%)
-- white blood cell count: 9100/µL (normal: 3500 to 12,500/µL)
-- erythrocyte sedimentation rate (ESR) 140 mm/h (normal: 0 to 20 mm/h)
Urinalysis results showed a trace of protein.
Results of randomly timed glucose testing were normal.
Physical Examination:Orthopedic: Pain was elicited by:
(1) palpation directly over the right sacroiliac joint and
(2) internal rotation of the right hip.
Neurologic: Examination of the lumbar spine and lower extremity produced normal results. Radiology:X-ray films initially obtained by the primary care physician were interpreted initially as showing normal anatomy.
Further review in the orthopedic clinic showed erosion at the inferior right sacroiliac joint (arrow) in the anteroposterior (AP) view shown below. An x-ray film of the patient’s lumbar spine showed only mild narrowing at L5-S1, as well as the abnormality of the right sacroiliac joint.
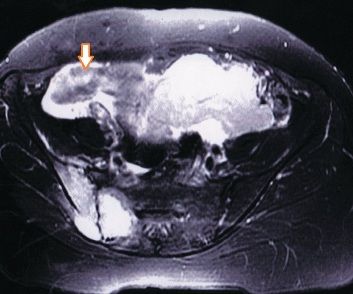
MRI scans of the pelvis (below) were interpreted initially as evidence of uterine sarcoma.


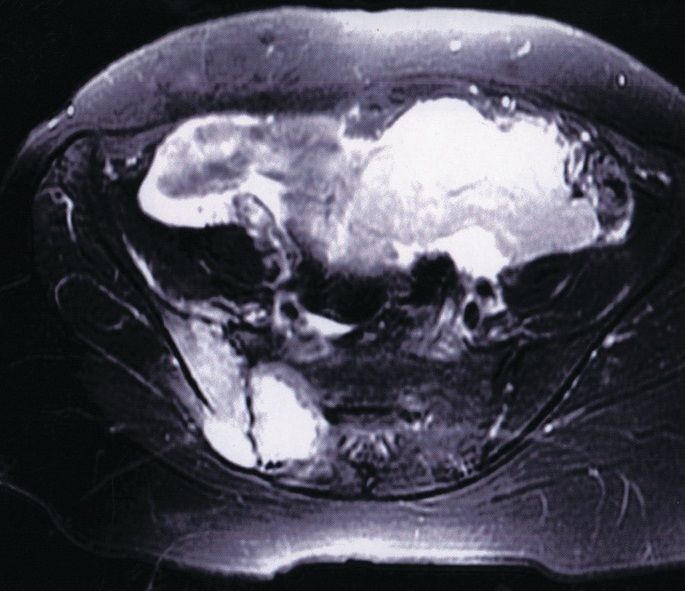



What do these images show?
What is your diagnosis?
Find the answer on the next page.
Multiple myeloma.
Retrospective review showed that the referrals to the orthopedic, gynecology, and dermatology clinics were all related to the same serious condition: multiple myeloma.
During outpatient evaluation for uterine sarcoma,laboratory test results confirmed a diagnosis of renal failure with hydronephrosis of the left kidney.
The patient was admitted to the hospital, where biopsy of both the pelvic lesion and the bone marrow yielded results consistent with multiple myeloma.
The MRI scan shown below left, a transverse cut through the pelvis, showed a solid lesion posteriorly and to the right (arrow). The other MRI scan (below right), a coronal cut through the pelvis, showed a solid lesion in much of the posterior pelvis (arrows).





Initially, this patient’s atypical presentation was confusing.The “hip pain” for which the patient was referred to the orthopedic clinic actually was a symptom of the sacroiliac lesion; neither the spine nor the spinal cord was affected.
A detailed discussion follows on the next page.
Discussion:
(References appear at the end of the final page.)
Multiple myeloma is the most common form of primary bone cancer;1,2 the median survival rate is 3 years.2
Plasmacytoma - the affected patient has only 1 lesion - is an early, isolated form of the disease, according to many researchers.1,2
Multiple myeloma may occur spontaneously, but it has been documented in patients who were exposed to ionizing radiation and various pesticides (eg, dioxin and dichloro-diphenyl-trichloroethane, or DDT).1,2 Diagnosis of about one third of new cases of multiple myeloma is made incidentally during evaluation for apparently unrelated problems.1,2
Multiple myeloma develops in the bone marrow and arises from malignant monoclonal plasma cells.2 The solitary form, plasmacytoma, occurs most often in persons younger than 40 years; the more typical (diffuse skeletal) form is observed most often in persons older than 40 years.3
In our patient, the presentation of multiple myeloma was unusual. Although she was a mail-order bride originally from Russia - prompting inquiry about possible exposure to radiation - she had neither lived in a Russian area with known radiation exposure nor received such exposure in the United States. In addition, subsequent diagnostic tests (eg, a skeletal survey) yielded normal results for every anatomic area other than the pelvis. However, the elevated ESR that was observed in this patient is a typical finding in multiple myeloma.
Outcome:
Our patient underwent aggressive disease management, including radiation therapy and dialysis.
However, she died 6 months after admission to the hospital.
This case was submitted by Janaleigh Hoffman,MD, a staff orthopedic surgeon in the department of orthopedics at Kaiser Permanente Medical Center in Fremont, California. Editorial assistance was provided by the Medical Editing Service of the Permanente Medical Group Physician Education and Development Department. (The report was further edited to adapt it to the quiz format on the Internet.)
References:
1. American Academy of Orthopaedic Surgeons. Multiple myeloma/plasmacytoma. Available at: http://orthoinfo.aaos.org/fact/thr_report.cfm?Thread_ID=488&topcategory=Tumors. Accessed August 22, 2006.2. George ED, Sadovsky R. Multiple myeloma: recognition and management. Am Fam Physician. 1999;59:1885-1894.3. Johnston JO, ed. Tumors. In: Johnson TR, Steinbach LS, eds. Essentials of Musculoskeletal Imaging. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 2003:144-146.














