Understanding Function in RA: Practical Evaluation in the Outpatient Setting
Observing rheumatoid arthritis patients in a systematic way allows rigorous analysis of pain and function. Learn how in this review.
ABSTRACT: A challenge with the aggressive new care model for patients with rheumatoid arthritis has been determining which measures to use to assess disease activity and response to therapy. With an observed functional assessment based on the Multidimensional Health Assessment Questionnaire domains, both the physician and the patient can gain important insights into function during a standard office visit. The presence of impairments in strength, joint range of motion, pain, and coordination-including balance and dexterity-can affect patients’ ability to perform functional activities. This assessment allows a physician to observe the impact of these impairments on function. It may help identify patients with significant changes in function who can benefit from effective intervention. (J Musculoskel Med. 2012;29:102-105)


Treatment of patients with rheumatoid arthritis (RA) has undergone tremendous advances related to greater understanding of its pathophysiology and the introduction of effective disease-modifying medications. New management strategies for RA use “treat to target” objectives with an intensive individualized approach and evidence-based outcomes.1,2
One challenge with this aggressive new care model has been determining which measures to use to assess disease activity and response to therapy. In the past, clinical assessment of joint swelling and tenderness, along with x-ray films and laboratory studies of acute phase reactants, formed the basis of the rheumatologist’s decision making. These tools provided perspectives about RA but offered limited information about the impact of synovitis on an individual patient’s function.
This is the fourth article in a 5-part series designed to provide a practical approach to better understanding of function in RA as an essential component of treat to target management strategies. The first article (“Understanding Function in RA: An Update on “Treat to Target,” The Journal of Musculoskeletal Medicine, February 2012, page 10) provided an overview. In the second article (“Understanding Function in RA: Importance and Measurement,” The Journal of Musculoskeletal Medicine, March 2012, page 41), we first presented a standardized vocabulary for describing function, based on the World Health Organization’s International Classification of Functioning, Disability and Health, and then applied it to an assessment tool frequently used in rheumatology, the Health Assessment Questionnaire (HAQ). The third article (“Understanding Function in RA: The Role of Impairments,” The Journal of Musculoskeletal Medicine, April 2012, page 78), described how impairments in body systems caused by RA can affect function and how patients can adapt their activities to cope with these impairments. This article discusses how functional assessment may be incorporated into clinical practice. The fifth article will describe the role of the nurse in multidisciplinary RA care.
ASSESSMENT OF FUNCTION
Information about function may be obtained in the following 3 ways: (1) asking the patient to self-report, using a questionnaire; (2) asking the patient directed questions; and (3) observing the patient perform activities. In 1980, Dr James Fries and the Stanford group introduced the HAQ, which provides a patient-centered self-report outcome tool that includes functional measures.3 The Multidimensional Health Assessment Questionnaire (MDHAQ),4 developed by Dr Theodore Pincus, is a modification of the HAQ; this tool includes the 8 function domains in the HAQ-dressing and grooming, arising (Figure), walking, eating, hygiene, reach, grip, and activities. This widely used self-report tool assesses standardized parameters of function. There is 1 question for each domain in the MDHAQ.
Research indicates that patient self-reports about function may have limitations.5 In addition, the clinician’s preconceived perspective of how a patient performs a particular task may be quite different from the actual performance.
With an observed functional assessment based on the MDHAQ domains, both the physician and the patient can gain important insights into function during a standard office visit. For the purpose of this assessment, the body is divided into 3 areas: upper body, trunk, and lower body. In some activities, such as turning on a faucet, the primary emphasis will be on 1 body area; other activities, such as picking up a shirt from the floor, require a combination of areas.
The presence of impairments in strength, joint range of motion, pain, and coordination-including balance and dexterity-can affect patients’ ability to perform functional activities. This assessment allows a physician to observe the impact of these impairments on function.
Before the evaluation, patients should complete the MDHAQ, which provides information about self-perceived performance of specific tasks. A physician, nurse, or other health care professional can perform the functional assessment in several minutes as part of the usual visit using items in a standard examination room plus a disposable cup.
To begin the assessment, the evaluator should ask the patient to sit in a straight-backed chair in an examination gown with shoes on. The examiner explains that as part of the visit, a brief functional assessment will be conducted to gain better understanding of how RA is affecting the patient’s day-to-day activities. “As part of your visit today, I want to evaluate how you perform certain basic activities. Let’s review your answers on the self-assessment form, and then you can show me how you do certain activities. If any are too difficult, or if you feel unsafe, let me know, and we can skip them.”
Patients generally become more engaged in the process when they specifically understand its purpose. Note that patients may answer “without any difficulty” to a question about an activity but actually may have a problem with it. During the examination, if patients are unable to perform an activity, ask, “What makes it difficult for you to do this?”
Dressing and Grooming
The first 2 activities address the domain of dressing and grooming. Begin by confirming that patients dress themselves at home and asking whether they have difficulty. You also may inquire whether they have made adaptations that make getting dressed easier, such as using a button hook tool, hook and loop fasteners, and a long-handled shoehorn.
Ask each patient to fasten 1 or 2 buttons on an article of clothing. If he or she is wearing a shirt, coat, or pants that have a button, use 1 of those buttons. If not, an extra laboratory jacket is an alternative.
Because buttoning is an in-hand manipulation activity that requires finger joint range of motion and dexterity to shift objects about, watch the patient’s hands carefully. Note that the buttons on women’s shirts are on the left and they use their left fingers to hold the button and their right fingers to open the buttonhole; men’s buttons are on the right side, and they are buttoned left over right. Either way, the patient should be able to place the button inside the hole smoothly and without repeated movements.
Also, note whether the patient shows signs of discomfort or pain. Avoid offering assistance in dressing or buttoning and other tasks so that you can make an accurate assessment of the patient’s abilities. If the patient struggles with the activity, ask how he manages at home, including whether he uses assistive devices.
Next, ask the patient to take off his shoes and put them back on. If the patient is wearing shoes that have laces, this activity should include tying them. Watch the fingers carefully-patients with RA may take more time positioning shoestrings. If the shoes do not have laces, ask the patient whether he has difficulty in tying shoes.
The knees, hips, and ankles also are involved with shoe tasks. Patients who have knee or hip swelling or range of motion abnormalities may slide their feet into shoes with or without laces rather than lift them. Observe whether the patient bends over to tie his shoes on the floor or crosses his legs and ties at waist level. Also, foot deformities may affect shoe activities and influence the patient’s preferred style of shoes.
Observing shoe activities can provide clues to patients’ difficulties with other dressing tasks that involve the lower body, such as putting on trousers and socks. Many patients with RA have developed safe, acceptable workaround strategies for dressing. If they are satisfied with their alternative and it poses no safety issues, no intervention is needed.
Arising
As part of assessment of the arising and activities domains, ask the patient to stand up from the chair. The patient should be wearing shoes, which is important for preventing slips and falls. Arising has the following 3 components: placing the feet in position, centering the body for balance, and lifting the body up. Each body area-upper, trunk, and lower-and the elements of strength, joint range of motion, pain, and coordination are part of this activity.
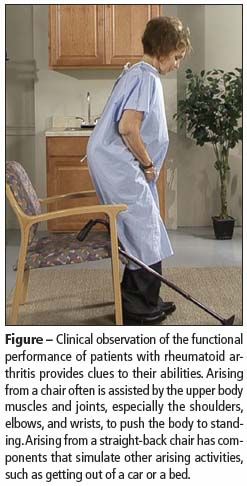
Watch carefully as the patient stands. Does he prepare to stand by inching toward the edge of the seat? Are his feet placed behind the edge of the chair before he moves forward and up? The knees must flex beyond 90° to facilitate moving the center of gravity of the upper body over the feet. The hip and knee extensor muscles then lift the body up. Arising often is assisted by the upper body muscles and joints, especially the shoulders, elbows, and wrists, to push the body to standing.
Other things to look for include the following: Does it take the patient more than 1 try to arise? Is the patient slow or deliberate in the process? Does he have expressions of pain or grimaces? Also, does he appear to be stable when he reaches the standing position?
Arising from a straight-back chair has components that simulate other arising activities, such as getting out of a car or a bed. Ask patients about these other activities. For example, when the patient arises from these other locations, are there issues with lower or upper extremity strength and range of motion? Can the patient twist his trunk and swing his legs to the side? How much does he use his upper extremities to pull himself up? The height of the car or bed and the depth of the car seat can affect performance-arising from higher surfaces is easier.
Walking
The next domain to be assessed is walking. Once the patient is standing, ask him to walk 5 steps and turn around and walk back. If the patient typically uses a cane or walker, ask him to use it to perform this task. Focus your attention on the patient’s lower extremities, and consider the smoothness, stability, and speed of his gait. Does he limp or favor one leg? Does he hold onto furniture and put a hand to the wall for balance? Does he exhibit signs of pain?
Now ask the patient to sit back down in the chair. Like standing, this task provides an excellent opportunity to observe the effect on functional activities of impairments in strength, joint range of motion, pain, and balance. Does the patient ease into the chair using his arms to steady himself? Does he have difficulty in bending his hips or knees? Does he fall into the seat? The components involved with sitting also have similarities with getting into a car and bed. You can take this opportunity to review these activities with the patient and note your observations.
More Dressing
The next activity helps you further assess dressing. Ask the patient to stand and take several steps forward. Then ask him to put on his shirt or coat. If he does not have one with him, simulate the activity. Observe the shoulders carefully-they have the greatest range of motion of any joint and are actively engaged in positioning the arms and hands when a shirt is donned, as are the elbow and wrist joints.
Hygiene and Reach
The next domains to be tested are hygiene and reach. Explain to the patient that you would like him to simulate washing and drying himself. Ask whether he bathes in a shower or tub and whether he stands or sits to wash and dry. Inquire how he bathes his back and front and upper and lower extremities.
Begin by asking the patient to place his hands on top of and then behind his head and simulate washing his hair. Ask him to put his hands to his shoulders, then behind his back, and then to the front.
Next, ask whether the patient can bend down to reach his knees or below. If yes, instruct him to pretend that he has a cloth and to slowly wash and dry his legs. Stand beside him and carefully watch for balance and stability, and immediately stop him if you sense that he is having difficulty.
When the patient is bent down, ask him to pretend to pick up a piece of clothing from the floor, which demonstrates reach and hand dexterity. Consider the speed and smoothness of the performance.
If the patient has limitations in bathing or reaching, ask whether he uses an adaptive device at home. If a patient can reach below his knees, to his lower back, and to his head, he probably can bathe himself and pick up clothing from the floor. You can take this opportunity to inquire about whether the patient has any issues with other personal hygiene activities.
Grip
While the patient is standing, ask him to go to the sink and turn the faucet on and off. This task helps in assessing grip. Focus attention on the distal upper body along with the shoulders, elbows, and forearms. The positioning of the fingers is particularly important in this task. Although patients with RA have joint impairments, many have developed effective adaptations to perform these kinds of daily activities.
While the patient is at the sink, ask him to fill a disposable cup from the faucet and lift it to his mouth. Do not hand him the cup; rather, ask him to pick it up from the sideboard or sink. Focus your attention on his hands and fingers. Notice how he lifts the cup. Does he grasp it with 1 or 2 hands? Are his fingers at the top or on the sides of the cup?
Patients with advanced RA may clamp the cup between their hands. Consider the speed and smoothness of the task when judging the efficiency of the performance. Does liquid spill from the cup? If the task seems manageable but awkward, ask how the patient feels about his performance. Is he satisfied? Is he embarrassed?
The disposable cup is different from other containers; the patient may report that he typically uses cups with handles. Difficulties with the faucet or cup activities may indicate other functional challenges with hand movements, such as picking up coins, opening car doors or jars, using a computer or cell phone, and writing.
Arising and Activities
The next activity includes some components of the arising and activities domains involving getting in and out of a car or bed. Begin by pulling out the step on the examination table. Ask the patient to stand facing the table and step up using the side of the table cushion or wall beside it as a simulated banister. This activity may be challenging. Immediately stop the patient if safety is an issue.
As the patient steps up, first focus your attention on movement in the lower extremities, including hip and knee flexion. Which foot does the patient first place on the step? Then note whether the patient uses his arms to pull the body forward. Upper and lower extremity strength, joint range of motion, and balance are integral to stepping up and onto the examination table. Assessment of this activity also may provide perspective on how well the patient can climb stairs.
Next, have the patient turn around on the step and sit at the end of the table for the final activity, which addresses bed mobility. Direct the patient to lie down and roll onto his side. Focus your attention initially on the upper body and trunk as the patient turns. Then, as he lies down, watch for smoothness, speed, and control of motion. Does it take more than 1 attempt? Are the patient’s arms and legs used to provide the strength to push the body over? Is the effort painful? Because this activity is performed on the examination table, it may serve as a natural segue into the physical examination.
SUMMARY
Clinical observation of patients’ performance with the use of this procedure provides the physician, other health care professionals, and patients with clues to their functional abilities, with an emphasis on personal care tasks and mobility issues. The assessment may help identify patients with significant changes in function who can benefit from effective intervention. This may mean altering medication prescriptions to better manage pain, stiffness, and inflammation, or it may mean referring the patient to an occupational therapist, the member of the health care team who specializes in the evaluation and management of function. The fifth and final article in this series will review the integrated multidisciplinary management of RA, with a focus on function.
References:
REFERENCES
1. Grigor C, Capell H, Stirling A, et al. Effect of a treatment strategy of tight control for rheumatoid arthritis (the TICORA study): a single-blind randomised controlled trial. Lancet. 2004;364:263-269.
2. Smolen JS, Aletaha D, Bijlsma JW, et al. Treating rheumatoid arthritis to target: recommendations of an international task force [published correction appears in Ann Rheum Dis. 2011;70:1519]. Ann Rheum Dis. 2010;69:631-637.
3. Bruce B, Fries JF. The Health Assessment Questionnaire (HAQ). Clin Exp Rheumatol. 2005;23(5 suppl 39):S14-S18.
4. Pincus T, Sokka T, Kautiainen H. Further development of a physical function scale on a MDHAQ [corrected] for standard care of patients with rheumatic diseases [published correction appears in J Rheumatol. 2005;32:2280]. J Rheumatol. 2005;32:1432-1439.
5. Carter JD, Lodhi AB, Nagda SR, et al. Determining rheumatologists’ accuracy at assessing functional disability in rheumatoid arthritis patients using the Health Assessment Questionnaire–Disability Index. J Rheumatol. 2007;34:958-963.














