Collaborative Primary Care Significantly Improves Depression Severity, Antidepressant Use
Depression patients monitored by physicians and care managers in a collaborative model have better antidepressant medication use and clinical outcomes than those treated in a traditional primary care setting, according to a comparison of the two delivery methods published in the May 2013 issue of Clinical Practice & Epidemiology in Mental Health.



Depression patients monitored by physicians and care managers in a collaborative model have better antidepressant medication use and clinical outcomes than those treated in a traditional primary care setting, according to a comparison of the two delivery methods published in the May 2013 issue of Clinical Practice & Epidemiology in Mental Health.
For their “Antidepressant Medication Use Among Patients with Depression: Comparison between Usual Care and Collaborative Care Using Care Managers” study, Ramona S. DeJesus, MD, and three colleagues from the Mayo Clinic in Rochester, MN, reviewed a year’s worth of medical records of 333 adult patients enrolled in the statewide Depression Improvement Across Minnesota Onward to New Direction (DIAMOND) program aimed at improving depression care in primary care settings. Within that study population, 242 depression patients — 50 percent of whom had been taking an antidepressant medication prior to enrollment — were registered under a collaborative care model (CCM) utilizing psychiatrist consultants who supervise care coordinators and make recommendations to primary care providers, while 91 patients were managed through usual practice.
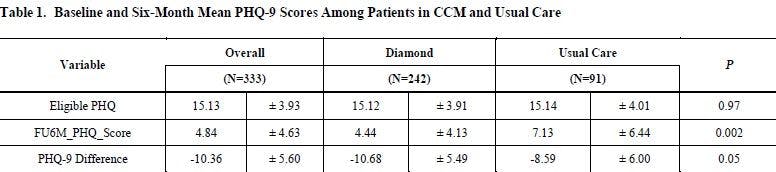
Though both groups shared an initial depression severity Patient Health Questionnaire-9 (PHQ-9) score of 15 at the time of enrollment, the mean PHQ-9 score of the CCM patients decreased to 4.44 after six months — a 71 percent reduction — while the usual care patients’ mean score only decreased to 7.13, the researchers said. (Table 1)


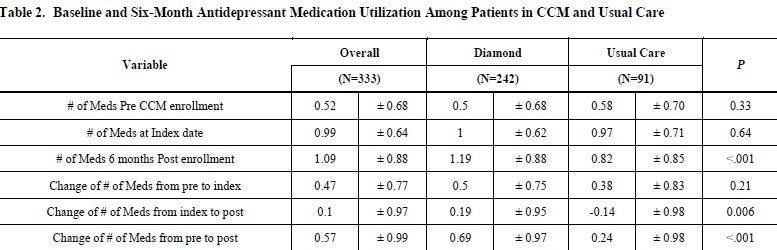
In addition to improvement in depression symptoms, the CCM patients had “significantly greater utilization of antidepressant medications at the end of six months (and) they likewise had more change in the number of medications from the index point or at the time of CCM enrollment to six months” — a result of more aggressive medication adjustments with closer follow-ups under CCM, the authors said. (Table 2)


Interestingly, a subset analysis of geriatric depression patients uncovered no significant difference in mean PHQ-9 score at six months or antidepressant use among those aged 65 years and older between the two study groups, though the investigators noted that “a larger sample of patients in this age group might yield a different result,” since their study only enrolled 35 subjects over the age of 65.
Regardless, the authors said their findings align with previous evidence from the National Institute of Mental Health-funded Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial — which “demonstrated that simply starting patients on antidepressant medications without care coordination only helped a third of these patients” — and they added that the results have “significant implications in depression management particularly among primary care settings” for achieving sustained clinical outcomes.
“Medication adjustment and changes in response to patients’ symptoms are hard to coordinate in usual practice, (but) under CCM, the care managers can bring forward treatment response issues to the attention of both the primary care physicians and collaborating psychiatrist so appropriate adjustments or changes can be made,” the authors concluded. “The CCM has been shown in various studies and systematic reviews to be consistently effective in depression management — both in achieving and maintaining remission — (and) results from this study showed similar findings.”













