Managing meniscal injuries: The diagnosis
First of two parts on diagnosis and management of meniscal injury, this reviews common tear patterns and elements of history, physical examination and imaging that lead to correct diagnosis.
The menisci are disks of fibrocartilage attached to the superior articular surface of the tibia. Injuries to the menisci are common and occur in persons of all ages and at all activity levels. The annual incidence of meniscal injury is 60 to 70 per 100,000 persons; the male to female ratio is 2.5-4:1.1
Meniscus damage often is associated with other injuries, such as anterior cruciate ligament (ACL) tears, tibial plateau fractures, and femoral shaft fractures. In fact, about 33% of meniscal tears are associated with ACL injuries, and 80% of repairable meniscal tears occur with ACL tears.2 The medial meniscus is more commonly torn than the lateral meniscus, and tears are more frequently located in the middle and posterior portions of the meniscus.
Diagnosis of meniscal pathology has improved with the use of MRI. Treatment has evolved dramatically with the use of arthroscopy and will continue to change as increased understanding of meniscus anatomy and function leads to the development and perfection of alternative treatment options.
In this 2-part article, we describe the diagnosis and management of meniscal injuries. This first part reviews the anatomy and function of the meniscus, common tear patterns, and the elements of the history, physical examination, and imaging that lead to the diagnosis. In the second part, to appear in a later issue of this journal, we will describe nonoperative and operative approaches to treatment.
ANATOMY AND FUNCTION
Anatomy
The medial and lateral compartments of the knee have intervening menisci located between the femur and tibia (Figure 1). The meniscal surfaces conform to the femoral and tibial contours. The medial and lateral menisci are peripherally thick and convex; they taper centrally to a thin, free margin. Both menisci have anterior and posterior bony attachment sites.
On a microscopic level, the menisci are fibrocartilaginous tissue composed of cells interspersed in a matrix of collagen bundles along with noncollagenous proteins, including elastin and proteoglycans. Two cell types are present: a more fusiform, fibroblastic cell and a more rounded, chondrocytic cell. Water constitutes 72% of the extracellular matrix, and collagen makes up 75% of the dry weight.3 Type I collagen represents 90% of the collagen present, and types II, III, IV, V, and VI make contributions that vary with location and age.

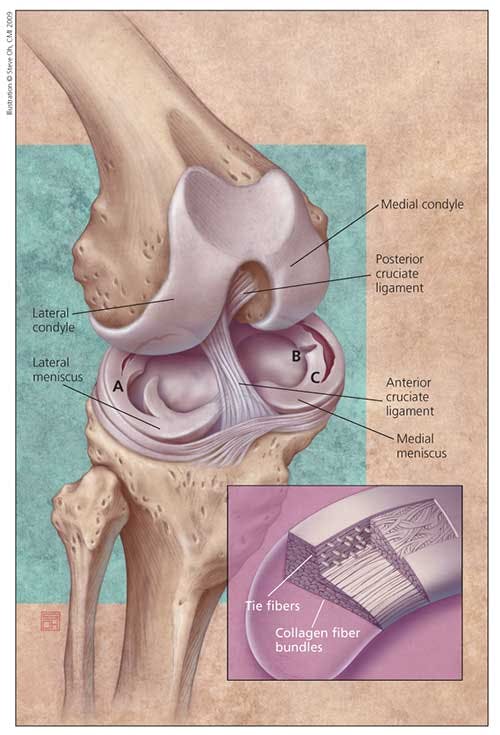
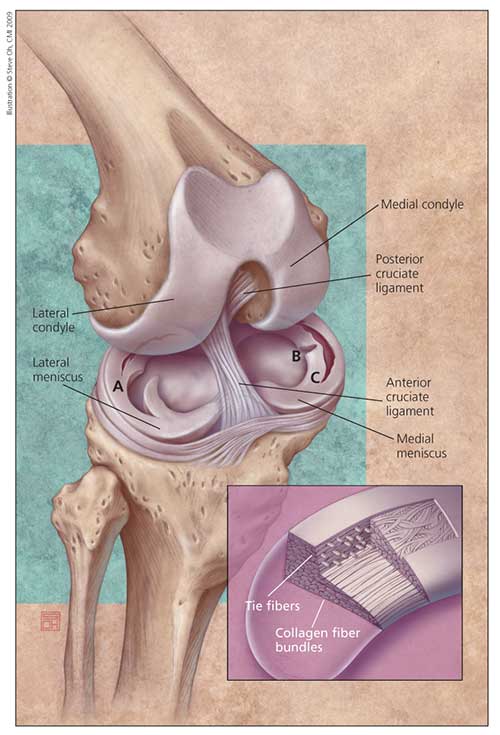
The principal orientation of collagen fiber bundles is a circumferential pattern (Figure 1, inset). The fiber bundles serve to absorb compressive loads. The circumferential nature of the type I collagen bundles affords tensile strength and is thought to be important in preventing radial extrusion of the meniscus during load bearing.4 In addition, radially oriented "tie fibers" provide structural rigidity to resist forces that would split the circumferential fibers with loading.1,3
Figure 1 – The menisci are located in the medial and lateral compartments of the knee. Their surfaces conform to the femoral and tibial contours. Both the medial meniscus and lateral meniscus have anterior and posterior bony attachment sites. Tears can result from trauma or degeneration. Common meniscal tear patterns (A, flap tear; B, radial tear; C, longitudinal tear) are shown. Collagen fiber bundles in the meniscus, which serve to absorb compressive loads, have a circumferential pattern, and radially oriented "tie fibers" provide structural rigidity (inset).
The medial and lateral menisci demonstrate an extensive microvascular network that arises from their respective superior and inferior geniculate arteries. The perimeniscal capillary plexus is oriented circumferentially, and it branches extensively into smaller vessels to supply the peripheral border of each meniscus. These capillaries coalesce into smaller vessels to supply the peripheral 10% to 30% of the menisci through attachment to the capsule. The remainder of the meniscus is avascular.2,5
Similarly, nerve fibers originate in the perimeniscal tissues and radiate into the peripheral 30% of the menisci. The most densely innervated regions are the anterior and posterior horns; these nerves are thought to play a proprioceptive role for protective neuromuscular reflex control of joint motion and loading.1
The medial and lateral menisci are identical in microanatomy, but their soft tissue attachments are different. The medial meniscus (about 3.5 cm long, semicircular, crescent-shaped, and wider posteriorly)5 covers 50% to 60% of the medial tibial plateau.6,7 The attachment site for the anterior horn is in the area of the intercondylar fossa, in front of the ACL. The posterior fibers of the anterior horn merge with the transverse fibers of the intermeniscal ligament (a structure that connects the anterior horns of the medial and lateral menisci) located about 8 mm anterior to the ACL.
The posterior intercondylar fossa, located anterior and medial to the posterior cruciate ligament, serves as the attachment site for the posterior horn of the medial meniscus.1 The periphery is attached to the knee capsule throughout its length. The deep medial collateral ligament (MCL), a condensation of the joint capsule, provides an additional firm attachment of the medial meniscus to the femur and tibia.6
The lateral meniscus (almost circular, nearly uniform in width from front to back) covers 70% to 80% of the lateral tibial plateau.5,6 Its bony attachments are much closer to each other than those of the medial meniscus. The anterior horn inserts adjacent to the ACL, and the posterior horn inserts just posterior to the ACL, anterior to the posterior horn of the medial meniscus. The lateral meniscus is loosely attached to the joint capsule; this allows for greater translation of the lateral meniscus than the firmly attached medial meniscus.5
Motion of the lateral meniscus is guided by the capsular attachments and additional ligamentous attachments, including the meniscofemoral ligaments (the ligaments of Humphry and Wrisberg), as well as the anteroinferior/posterosuperior popliteomeniscal fascicles from the popliteus muscle. The guided motion provided by these ligaments may play a protective role in avoiding injury.8
Biomechanics and function
The menisci serve in load transmission, shock absorption, lubrication, prevention of synovial impingement, synovial fluid distribution, stability, improved gliding motion, and articular cartilage nutrition.1,3,6,7,9 The medial meniscus has a greater role in stability, and the lateral meniscus contributes more to load transmission.9 As much as 50% to 70% of compressive load is transmitted through the menisci in extension, and 85% is transmitted at 90° of flexion.1,2,5,6 After total meniscectomy, degenerative changes develop in virtually all knees.10 Removal of any portion of the meniscus results in increased bony contact area between the femur and tibia. In fact, resection of as little as 15% to 34% of the meniscus results in increased contact pressure up to 350%11; this can lead to progressive degenerative changes that resemble those of osteoarthritis.5
With knee flexion from 0° to 120°, the menisci move posteriorly. In the midcondylar, parasagittal plane, the medial meniscus moves about 5.1 mm and the lateral meniscus moves 11.2 mm.5 Posterior motion of the medial meniscus is guided by the deep MCL and semimembranosus; anterior translation is caused by the push of the anterior femoral condyle.11
Because the posterior oblique fibers of the deep MCL limit motion in rotation, the medial meniscus is at increased risk for tearing. The lateral meniscus motion is guided by the popliteus tendon, popliteomeniscal ligaments, meniscofemoral ligaments, and lateral capsule. The more controlled motion may provide escape of the lateral meniscus from injury. Meniscal motion allows continued load distribution during changes of position of the joint when the radius of curvature of the femoral condyles changes.11
The menisci serve as secondary restraints for knee stability. Although the menisci deepen the plateaus only slightly, this deepening provides for a more congruent and constrained surface with the femoral condyles.11 The medial meniscus provides greater restraint to anterior translation than the lateral meniscus because it is more rigidly attached.
The medial meniscus is considered a secondary restraint to anterior tibia translation. An ACL-deficient knee that has also required medial meniscectomy demonstrates increased anterior tibial translation at all angles of flexion when compared with an ACL-deficient knee that has intact menisci.12 In meniscus-intact knees, with sufficient anterior translation, the posterior horn of the medial meniscus becomes wedged between the tibial plateau and the femoral condyle and provides resistance to translation. In ACL-deficient knees, the soft tissue attachments of the lateral meniscus do not affix the lateral meniscus as firmly to the tibia; more mobility results in a decreased resisting force to anterior translation.13 Thus, the lateral meniscus provides little help as a secondary restraint to anterior translation.
Tear patterns
Meniscus injuries can be classified according to the description of tear pattern (see Figure 1). Patterns include vertical, longitudinal, horizontal, oblique (eg, flap, parrot-beak), radial (transverse), and complex tears. About 80% of tears have a vertical or oblique pattern.1
Medial meniscus tear patterns are more commonly longitudinal; radial tears occur more frequently in the lateral meniscus.2 Radial tears disrupt the circumferential fibers of the meniscus and result in loss of the load-bearing function of the involved portion of the meniscus. A complete displaced vertical tear (bucket-handle tear) can result in a mechanical block to motion.
Meniscal tears also can be classified as traumatic or degenerative. Most tears are degenerative; they occur without significant trauma and may not be associated with a recalled event. Overall, degenerative tears increase in frequency with patient age. In men, they peak in frequency in the fourth through sixth decades; in women, the frequency remains somewhat constant after the second decade.1
A normal meniscus is formed by circumferential collagen bundles and converts axial loads to hoop stresses. Disruption of the circumferential fibers by a meniscus tear results in the loss of function and an increase in forces seen by the articular cartilage. Meniscal tears result in flaps of meniscal tissue that may be unstable and responsible for the majority of symptoms that the patient experiences. Any torn portion of the meniscus will have lost the ability to form hoop stresses and is considered nonfunctional. Resection of this portion of unstable meniscus does not result in further loss of meniscal function.
DIAGNOSIS
History
Along with MRI, the history and physical examination remain the primary methods of making the diagnosis of meniscal pathology. Usually, a patient's description of the injury, if recalled, and symptoms guides the physician to the diagnosis. Injury to the meniscus during sports activity frequently occurs during noncontact cutting, deceleration, hyperflexion, or landing from a jump. Often, degenerative injury that occurs with aging (older than 40 years) does so after trivial insult. The tear may not be noted at the time of injury, but the symptoms that follow often trigger the patient to seek attention.
The complete history should include assessment of the patient's lifestyle, activity level, occupation, and medical history. Younger, more active persons often require more aggressive management.
Mechanical symptoms that are suggestive of meniscal tear include popping, catching, locking, and buckling, along with joint-line pain. These symptoms are nonspecific and may also be the result of chondral injury, ligament tear, patellofemoral chondrosis, or synovitis.1 Synovitis may result from meniscus injury and lead to the development of a delayed effusion several days after the event. The synovitis that results may be recurrent and activity-related.
An audible pop at the time of injury is more characteristic of an ACL tear, but a meniscus tear often is also present in this scenario. Immediate swelling suggests bleeding; frequently, swelling is not initially present after an isolated meniscus tear, but it may be present with a peripherally based tear. In addition, swelling may develop several days after a meniscus tear as a synovitis is produced from mechanical irritation.
Loss of motion accompanied by a sensation of a mechanical block to extension is suggestive of a displaced meniscus tear.1 Displaced tears may be reduced successfully after an intra-articular injection of anesthetic to provide pain relief and relaxation. If this is not accomplished, arthroscopy is required for meniscectomy or meniscal repair, depending on the tear pattern. A history of a snapping or popping knee, especially in childhood or adolescence, should raise suspicion of a diskoid meniscus (a variant found more commonly in the lateral compartment).6 This meniscus variant, which occurs in about 5% of the population, represents a meniscus that covers a larger percentage of the weight-bearing surface of the tibia. Rather than the normal crescent shape, the diskoid meniscus is virtually solid, thickened, and circular.
Physical examination
Examination begins with noting of the patient's gait. A limp is common after a meniscus tear; if the injury is acute, the patient may not be able to bear weight fully.
Inspection of the knee includes evaluation for an effusion and for thigh asymmetry in the setting of a chronic tear. The joint lines should be palpated; the presence of tenderness may be the best clinical sign of a tear (74% sensitivity and 50% positive predictive value).1
Cysts at or below the joint line may be palpable (more commonly lateral) and are highly correlated with meniscal tears.1 Any cause for increased synovial fluid production, including a meniscal tear, can result in development of a popliteal cyst. Posterior horn meniscal tears that extend to the capsule may cause a defect posteromedially between it and the medial head of the gastrocnemius or semimembranosus muscles. This communication allows for egress of joint fluid and the creation of a popliteal (Baker) cyst.
Range of motion is tested, and the results are compared with those of the contralateral side. A displaced tear may block extension or flexion or both. A mechanical block to motion, termed a "locked knee," may be present. The examiner should take particular note of pain elicited during terminal range of motion.
The most common test for meniscal pathology is the McMurray sign. This test is performed with the patient supine and the hip and knee flexed. The patient's foot is alternately rotated internally and externally during application of a circumduction maneuver to the knee. At the same time, the examiner palpates the posterolateral and posteromedial joint lines. Medial and lateral meniscal injuries are tested by extending the knee with the foot externally and internally rotated, respectively. A palpable or audible clunk is considered a positive McMurray sign. A true positive sign is uncommon, even in the presence of a tear, but, when present, it is nearly 100% specific.1 The sensitivity of the test is as low as 15%. Circumduction testing more commonly elicits pain.13 Pain with this maneuver is sensitive yet not, by definition, a true positive McMurray sign.
The presence of a meniscal tear also may be detected with the Thessaly test. In this test, the patient internally and externally rotates through the knee while standing flatfooted on the symptomatic leg only; this is done with the knee in 5° and 20° of flexion. The Thessaly test is designed to dynamically load the knee and engage the unstable meniscal tear. A positive test result is one in which joint-line discomfort is elicited. There may be a sense of locking or catching as the tear is engaged. The test was found to have a sensitivity of 89% to 92%, with a specificity of 97% to 96%.14
No one clinical examination finding is diagnostic of a meniscal tear, but the combination of several positive test results (eg, joint-line tenderness, pain on forced flexion, positive McMurray sign, positive Thessaly test result, and a block to extension) is highly predictive. Sensitivity and specificity of a thorough examination can be as high as 95% and 72%, respectively.1
Diagnostic imaging
Imaging should always begin with plain radiography for assessment of loose bodies, associated skeletal injury, and degenerative changes. X-ray films should be obtained during weight bearing. They should include a 45° flexion view to allow for evaluation of the posterior tibiofemoral contact region, which frequently is involved in early degenerative arthritis. Lateral joint-space widening, cupping of the lateral tibial plateau, or flattening of the lateral femoral condyle suggests a diskoid meniscus.



Figure 2 – This sagittal MRI scan depicts a grade 3 signal change within the medial meniscus (arrow) that is consistent with a tear.
MRI is the imaging modality of choice for evaluation of the menisci (Figures 2 and 3); accuracy of detection of meniscal tears approaches 95%.1 However, misinterpretation of normal structures, such as the intermeniscal ligament and the popliteus tendon hiatus, can lead to false-positive results. Interpretation of MRI can be confusing, because the meniscus is not always homogeneous; interpreting MRI results in knees that have previously undergone meniscectomy is particularly difficult. Ciliz and associates15 have shown that MR arthrography has improved sensitivity and specificity when compared with conventional MRI for detection of recurrent meniscal tears after arthroscopic surgery.

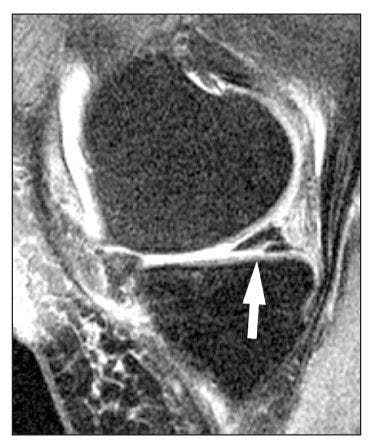

Figure 3 – In this coronal MRI scan, a grade 3 signal change within the medial meniscus (arrow) consistent with a tear is shown.
Altered signals do not necessarily represent gross pathology (Table). In fact, abnormal signal has been found in up to 30% of asymptomatic patients who did not have a history of knee injury.6 A finding of solid meniscal tissue on 3 or more contiguous sagittal cuts suggests a diskoid meniscus. False-positive results occur more frequently than false-negative results, thus emphasizing the need

for clinical correlation.
Judicious use of MRI is recommended in patients in whom arthroscopic surgery is anticipated. Routine MRI does not significantly improve diagnostic accuracy compared with clinical examination alone.16 However, MRI does provide information about the extent of the tear and helps identify occult chondral and osseous injuries.

The threshold for obtaining an MRI scan is physician-dependent. However, a low threshold should be applied for younger patients with the suggestion of meniscus pathology on clinical examination, because these patients are more likely to benefit from early surgical intervention. In lower-demand patients or in patients in whom a tear probably is degenerative, a period of observation or therapy or both is appropriate. If plain radiographs do not show signs of degenerative arthritis, a shorter period of observation is warranted.
References:
References1. Greis PE, Bardana DD, Holmstrom MC, Burks RT. Meniscal injury, I: basic science and evaluation. J Am Acad Orthop Surg. 2002;10:168-176.
2. Klimkiewicz JJ, Shaffer B. Meniscal surgery 2002 update: indications and techniques for resection, repair, regeneration, and replacement. Arthroscopy. 2002;18:14-25.
3. Fairbank TJ. Knee joint changes after meniscectomy. J Bone Joint Surg. 1948;30B:664-670.
4. van Tienen TG, Hannink G, Buma P. Meniscus replacement using synthetic materials. Clin Sports Med. 2009;28:143-156.
5. Arnoczky SP, McDevitt CA. The meniscus: structure, function, repair, and replacement. In: Buckwalter JA, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2000:531-545.
6. Rath E, Richmond JC. The menisci: basic science and advances in treatment. Br J Sports Med. 2000;34:252-257.
7. Lo IK, Thornton G, Miniaci A, et al. Structure and function of diarthrodial joints. In: McGinty JB, ed. Operative Arthroscopy. 3rd ed. Philadelphia: Lippincott, Williams and Wilkins; 2003:41-126.
8. Greis PE, Holmstrom MC, Bardana DD, Burks RT. Meniscal injury, II: management. J Am Acad Orthop Surg. 2002;10:177-187.
9. Packer JD, Rodeo SA. Meniscal allograft transplantation. Clin Sports Med. 2009:28:259-283, viii.
10. Andersson-Molina H, Karlsson H, Rockborn P. Arthroscopic partial and total meniscectomy: a long-term follow-up study with matched controls. Arthroscopy. 2002;18:183-189.
11. Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2000:730-827.
12. Levy IM, Torzilli PA, Warren RF. The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg. 1982;64A:883-888.
13. Levy IM, Torzilli PA, Gould JD, Warren RF. The effect of lateral meniscectomy on motion of the knee. J Bone Joint Surg. 1989;71A:401-406.
14. Karachalios T, Hantes M, Zibis AH, et al. Diagnostic accuracy of a new clinical test (the Thessaly test) for early detection of meniscal tears. J Bone Joint Surg. 2005;87A:955-962.
15. Ciliz D, Ciliz A, Elverici E, et al. Evaluation of post-operative menisci with MR arthrography and routine conventional MRI. Clin Imaging. 2008;32:212-219.
16. Miller GK. A prospective study comparing the accuracy of the clinical diagnosis of meniscus tear with magnetic resonance imaging and its effect on clinical outcome. Arthroscopy. 1996;12:406-413.











 May Offer Over PPIs, with Adelina Hung, MD")



