
Commentary|Videos|September 22, 2023
Patient Communication and Shared Decision Making
Author(s)Mark Barakat, MD
Mark Barakat, MD, reviews the best practices for patient communication and shared decision making.
Advertisement


Transcript
Mark Barakat, MD:And so before we go further, what's shared decision-making? It's basically the health provider and the patient have to work together to come up with a decision that's not best for the clinic, it's not best for the provider, it's best for the patient. And it's really all about knowledge. The knowledge base that we have is on the medical side. The knowledge base that the patient has is on the cultural, on the socioeconomic aspects, on values. All those things have to come together. We're going to talk about this a little bit more detail later on, but this is the SHARE approach. There are 5 steps: seek your patient's participation, help your patient explore and compare treatment options, assess your values for the patient, the preferences, then reach a decision. But don't forget step five. Every now and then you got to step back and evaluate the decision and see where we stand. And this is based on these 9 essential elements, you have to look at the problem, you have to present options, risk benefits, costs, values of the patient's preferences, the ability, self-efficacy of the patient, the recommendations, of course, the medical recommendations, right? Are you sure the patient's understanding? And then you make a decision and then you arrange for follow-up and re-evaluation.
But, again, why? We're here to talk about the data, right? Why do we care? We're busy. We're seeing a million patients. Why do we care? Because it helps everybody. It improves the patient's experience. It makes them more likely to adhere to treatment, to follow-up, to not get lost to follow-up. It increases the quality of care delivered and it increases the patient satisfaction. Well, great. That's wonderful for the patient. That in and of itself should be reason enough to do it. But frankly, it's good for the clinic, too. And I found this really interesting, because I am probably guilty of this. Many healthcare providers believe patients are not interested in participating in the decision-making process. There's actually this literature that suggests that patients actually want more information than they're typically given. Many of them would want to be more involved with the caveat that we all have that patient that does not want to, or is not ready to be part of the decision-making process. And, you know, that's something that we're respected. You will get that patient that says, “Doc, whatever you think is best for me, go ahead and do that.” That in and of itself is a decision, too. But on average, many people want more information than we think.
Well, how do we do this? Well, we were talking about the SHARE approach. Step 1, seek your patient's participation. That's probably the easiest thing to do. “Hey, do you want to be in a dialogue?” “Do you want to be involved in making this decision?” Or, do you fall into that category of, “Hey, doc, do what's best for me?” Start the dialogue. Step 2 is risk-benefits alternatives. That's an important consent in my mind. Discuss the benefits and harms of each option. We do this all the time. Sometimes a little bit more thoroughly than others. Possibly depending on how many patients you're seeing that day. But risk -benefits alternatives. Step 3, this is where it gets interesting. This is where we may not have the time or the training to do as well as we otherwise might. Assess your patient's values and preferences, and if they are taking into account what matters most to them. Now, I think many times, right now, specials do a great job with that. For example, if you have a patient with wet macular generation, you have this form of scar. And I'm willing to bet you have patients that say, “I don't care if I have this form of scar. I understand that it's not going to get any better. But I'm worried that it might get a little bit bigger. Keep going.” Or, if other patients say, “I don't want to keep going. That's not my decision.” That's their values, right? And we have that discussion all the time.
Then step 4, you reach a decision. And step 5, every now and again: “Okay, Ms. Jones, you've decided to keep injecting that this form of scar. We've been doing it for X number of months. Are you still happy with that? Do you see a difference?” You got to reevaluate it now and then it's not carved in stone. Patient buy-in is really essential to adherence. Now, without belaboring this anymore, there's so much more. This, this in and of itself could be like a 10-hour talk. But we do want to touch on just a few hurdles, because it seems so easy when you think about it. But there's more than a few hurdles. One, language, hearing, eyesight; [these are] common barriers. We all know about the vision. That's why we're here. But 9 out of a 100 limited English proficiency; 2 out of a hundred visual disability, 3% hearing disability, qualified medical interpreters. We have a bevy of qualified medical interpreters, which are listed here. Now, having a family members translate is probably not the best idea. And so that is one thing that we need to think about: health literacy. Twelve percent of US adults age 16 and older have proficient reading skills. Thirty-six percent of the population lack adequate literacy skills. And [that’s] for all ages, races, and income. So how can you get informed consent? It's really a conundrum that needs to be addressed. The impact is disproportionate. It affects lower socioeconomic and minority groups more so than it does others, so you have to keep that in mind. And here's the kicker: Nearly 9 out of 10 adults lack full literacy and have difficulty using everyday health information. It's shifting gears and trying to understand where the patients [are] coming from. Because here's the reason why: they are more likely to skip tests, underuse healthcare, to visit the emergency room, be hospitalized, not comply with treatment plan, etc.
The issue is patient buy-in. Here's some of the strategies. Unlike me, you should probably speak slowly and not rush through everything. Show some empathy. Avoid medical jargon. I think I'm as guilty of that as the next person, right? You're using plain language. The teach-back technique, I think is wonderful. It just takes a lot of time asking, “Hey, Mrs. Jones, what did I just tell you? What did we agree on?” That's hard, but it may be worth it, putting that effort in that first time and then read the benefits.
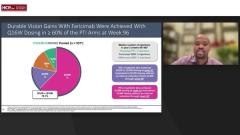
I think we're all really good at thinking about literacy, but what is numeracy? The ability to use numeric information in the context of health; it is also limited. Have you ever had a discussion with a patient and say, “Well, there's a 1 in 4,000 risk of [a certain side effect] or there's a 0.5% risk of [another side effect]?” And do you ever get that look [when you know you’ve] lost them. That's exactly what it is, because you need to understand numbers when choosing treatments, when weighing the risks and the benefits, right? If Matt and I were all happy, we’re thrilled, if close to 80% of patients can go up to Q12 to Q16 weeks. That’s a lot of numbers coming at you. You need these numbers for a bevy of tasks that are shown here. Here are some of the strategies. Frankly, use them only when you need them. When you need precision, use everyday words and approximations; [for example,] say “about one half” instead of 48%. You can elaborate for providing estimate numbers. Visual aids are great. Absolute risk instead of relative risk. That's a beautiful one, right? If you say, well, there's an additional small risk of X% and I do this all the time, just say, well, it's a tiny percent additional risk.
Transcript is AI-generated and edited for clarity and readability.
Advertisement
Related Content



Latest CME




































































Advertisement
Advertisement
Trending on HCPLive
1
Tirzepatide Demonstrates Cardioprotective Effects in T2D With ASCVD
2
Phase 3 Dermatomyositis Trial Sees Brepocitinib Meet Primary Endpoint
3
Socrodeucitinib Meets Primary Endpoint in Phase 2 Psoriasis Study
4
Omalizumab-Facilitated OIT Enables Maintenance Dosing in Food Allergy
5