Recommendation Against Screening for CHD With Resting and Exercise ECG in Asymptomatic and Low-Risk Adults
Review
Moyer VA, on behalf of the US Preventive Services Task Force. Screening for coronary heart disease with electrocardiography: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(7). Published online July 31, 2012. doi:10.7326/0003-4819-157-7-201210020-00514.

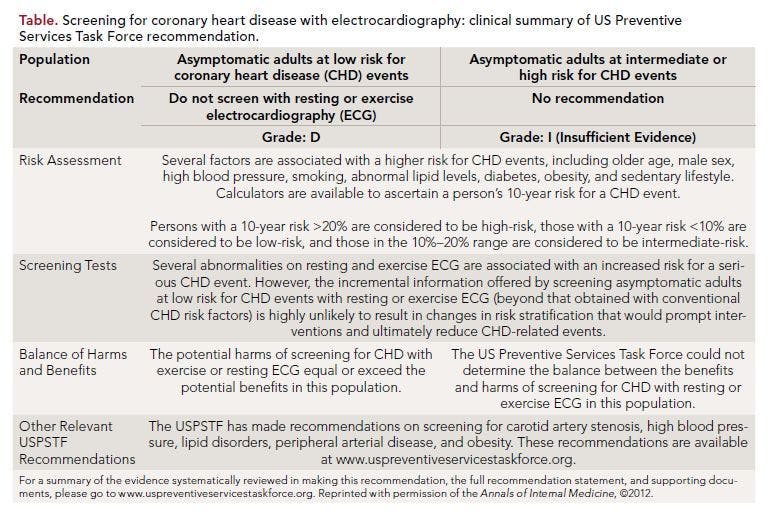
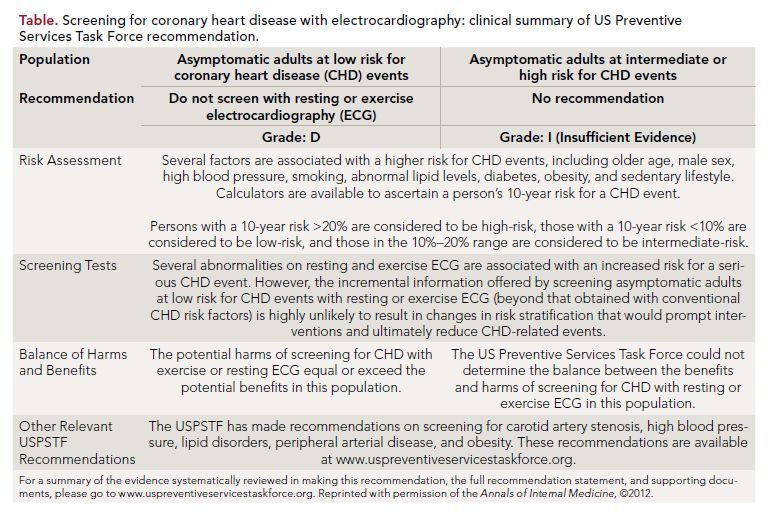
Moyer et al,1 on behalf of the US Preventive Services Task Force (USPSTF), present an updated recommendation statement on screening for coronary heart disease (CHD) with electrocardiography (ECG) in adults. The authors reviewed new evidence on the utility of screening with ECG in asymptomatic adults to attempt to favorably modify the risk for CHD events versus not screening, the possibility of identifying high-risk persons for treatment to reduce risk, the accuracy of stratifying individuals into risk categories, and the possible harms of screening. The document provides important insights into a clinically relevant issue.

In its 2010 guidelines, the American Heart Association/American College of Cardiology (AHA/ACC) gave a Class IIa recommendation for the evaluation of asymptomatic persons with diabetes or hypertension with a resting ECG. They also recommended consideration of an exercise ECG for cardiovascular risk assessment in intermediate- risk asymptomatic adults (including sedentary adults considering starting a vigorous exercise program), particularly when attention is paid to non-ECG markers such as exercise capacity, with a class IIb recommendation.2
The USPSTF did find adequate evidence that many resting and exercise ECG abnormalities were associated with an increased risk for a serious CHD event, even after controlling for conventional risk factors. The guidelines committee reports that it objectively weighed the evidence for benefits and harms of detection and early intervention. The major basis for their recommendation reportedly was a systematic review of the topic published in 2011.3 The authors of the USPSTF guidelines did find with “moderate certainty” that for adult women and men the possibility of harm associated with screening for CHD with exercise or resting ECG equaled or exceeded the potential beneï¬ts in asymptomatic adults at low risk for CHD events, as assessed with traditional risk factors (Grade D recommendation). The USPSTF also concluded that evidence was lacking, and that the balance of benefits and harms of screening for CHD with exercise or resting ECG in asymptomatic adults at intermediate or high risk for CHD events could not be determined on the basis of evidence reviewed by the committee (given an I statement, indicating insufficient evidence).

References
1. Moyer VA; on behalf of the US Preventive Services Task Force. Screening for coronary heart disease with electrocardiography: U.S. Preventive Services Task Force Recommendation Statement. [published online ahead of print July 31, 2012] Ann Intern Med. 2012;157(7). doi:10.7326/0003- 4819-157-7-201210020-00514.
2. Greenland P, Alpert JS, Beller GA, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: executive summary: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122:2748-2764.
3. Chou R, Arora B, Dana T, Fu R, Walker M, Humphrey L. Screening asymptomatic dults for coronary heart disease with resting or exercise electrocardiography: systematic review to update the 2004 U.S. Preventive Services Task Force Recommendation. Evidence Syntheses, No. 88. Rockville, MD: Agency for Healthcare Research
and Quality (US), September 2011. http://www.ncbi.nlm.nih.gov/books/NBK63671.Accessed August 20, 2012.
4. American Academy of Family Physicians. Recommendations for clinical preventive
services: coronary heart disease. Leawood, KS: AAFP, 2004. www.aafp.org/ online/en/home/clinical/exam/coronaryheartdisease. html. Accessed August 19, 2012.
5. Myers J, Arena R, Franklin B, et al; American Heart Association Committee on Exercise, Cardiac Rehabilitation, and Prevention of the Council on Clinical Cardiology, the Council on Nutrition, Physical Activity, and Metabolism, and the Council on Cardiovascular Nursing. Recommendations for clinical exercise laboratories: a scientiï¬c statement from the American Heart Association. Circulation. 2009;119:3144-3161.
Commentary
ECG Screening in Asymptomatic and Low-Risk Adults
Moyer et al present us with recommendations against screening of asymptomatic adults with resting or exercise ECG for possible reduction of CHD events. They also state that the available evidence was inconclusive to determine the balance of benefits and harms of screening with resting or exercise ECG for the prediction of CHD events in asymptomatic adults at intermediate or high risk for CHD events. Their conclusions appear to be largely congruent with other guidelines.
2,4 However, a few interesting issues merit deliberation:
1. The systematic review that the guideline authors have used as the basis of their recommendations actually concluded that “abnormalities on resting or exercise ECG are associated with an increased risk of subsequent cardiovascular events after adjusting for traditional risk factors, but the clinical implications of these findings are unclear.”3 The authors of the recommendations do refer briefly to that fact in their publication; however, they justify their recommendation against screening asymptomatic patients by stating that resting or exercise ECGs did not provide additional information about CHD risk beyond that obtained with the conventional Framingham risk factors, and did not result
in changes in risk stratiï¬cation and did not ultimately reduce CHD-related events. However, with findings of 80% to 100% increased relative risk in patients screened with resting or exercise ECGs,3 the consequences of completely abandoning a strategy of screening may not be optimal and remain open to debate.

2. On evaluating potential harms of screening, the authors vouchsafed that risks associated with performance of resting ECGs were minimal and restricted to allergic reactions to the ECG pads or adhesives and anxiety. Adverse events associated with exercise ECG might induce a cardiovascular event or musculoskeletal damage, along with anxiety about test/outcome. The overall risk for a serious adverse event (one that requires hospitalization or causes sudden death) was estimated to be 1 in 10,000 tests.5 The risks associated with later invasive confirmatory tests like angiography were deemed to be more significant, although numerically very small in absolute numbers. However, no comparative estimates in terms of absolute numbers (such as number needed to treat/harm), were provided by the authors for independent assessment by medical practitioners. Also, a brief mention of cost burden was referred to, but without presentation of a formal cost-effectiveness analysis.
3. Brief mention by the authors about potentially preventable disease burden, at least in some adults with intermediate to high risk and certain occupations that may jeopardize public safety, seems to indicate a direction for further research and the need for specific trials to assess if resting or exercise ECGs in suitable subjects led to risk restratification.
4. The authors considered only studies published in English and completely omitted unpublished studies and abstracts, which may have led to the omission of relevant studies and data—especially for a country with an ethnically diverse population.
In summary, the authors recommend against screening with resting or exercise ECG in asymptomatic adult patients at low risk of CHD events, and they did not find convincing evidence to recommend for or against such screening in high-risk individuals. Future studies are thus urgently needed to identify patients in whom such screening may lead to significant reduction in CHD events and to identify tools for appropriate risk-restratifications.
About the Author
Saurav Chatterjee, MD, is Clinical and Research Fellow in Preventive Cardiology and Outcomes Research at Brown University and Providence VAMC in Providence, RI. He graduated from Calcutta National Medical College with honors and was a Resident in Cardiology at Mercy Hospital, Kolkata, India, as well as trial coordinator of the CRESCENDO trial in Kolkata, India. He recently finished his residency in Internal Medicine at Maimonides Medical Center in Brooklyn, NY. Dr Chatterjee is the recipient of the
2012 Young Investigator Award for Health Outcomes and Population Genetics at the Annual Scientific Sessions of the American College of Cardiology 2012 in Chicago, and also the 2011 American Association of Cardiologists of Indian Origin (AACIO) Young Investigator Award for Interventional Cardiology and Electrophysiology.



