Risk assessment and prevention of arm injuries in baseball players
Although baseball is considered a generally safe sport, young pitchers often experience arm injuries. The repetitive nature of pitching makes the throwing arm susceptible to injury, particularly the elbow and shoulder.1 Microtrauma to soft tissue often is either without symptoms or mild, merely resulting in temporary pain and soreness. With continued stress, however, microtrauma may accumulate, thus increasing the probability of a serious injury.
Although baseball is considered a generally safe sport, young pitchers often experience arm injuries. The repetitive nature of pitching makes the throwing arm susceptible to injury, particularly the elbow and shoulder.1 Microtrauma to soft tissue often is either without symptoms or mild, merely resulting in temporary pain and soreness. With continued stress, however, microtrauma may accumulate, thus increasing the probability of a serious injury.
This problem can best be illustrated when its scope is placed in perspective. There are more than 12 million amateur baseball players, mostly children and adolescents, according to USA Baseball.2 Perhaps the most recognizable youth baseball organization, Little League Inc, oversaw 2.6 million players during the 2006 season.3 Nearly one-fourth of youth baseball players are estimated to participate as pitchers, translating into millions of young pitchers.
The enormous number of children and young adults who are at high risk for throwing arm injuries highlights the importance of prevention and treatment. A working knowledge of the risks is critical to physicians who are directly involved with these players, as well as parents and coaches, to keep them healthy and able to participate. In this article, we describe the main risk factors for throwing injuries in young athletes and ways to minimize and prevent these injuries.
RISK FACTORS
In a 2001 survey of Little League pitchers, 26% experienced elbow pain during the season and 32% had an episode of shoulder pain.4 Arm fatigue during the game was a risk factor for pain in both the shoulder and elbow. Throwing more than 75 pitches in the game was a shoulder-specific risk factor; pitching on an additional team and weight lifting during the season were risk factors for elbow pain.
An odds ratio for injury is provided by a 2006 follow-up study that compared injured adolescent pitchers with uninjured controls.5 Pitching in more than 8 months of the year, throwing more than 80 pitches in a game, and pitching with fatigue increased the risk of a shoulder or elbow injury more than 3-fold.5 Official USA Baseball recommendations have been based on studies such as these.
Pitching on a mound places more stress on the arm than pitching on flat ground.6 Basically, young athletes pitch too much and do not throw enough. Pitching involves the increased force of gravity when the pitcher strides off the mound and includes maximal stride length and rotational torques on the shoulder and elbow; throwing on flat ground does not place the same stresses on the arm. Therefore, year-round throwing is acceptable because it facilitates endurance, adaptation, and accommodation to the movement. However, year-round pitching is not acceptable because it exacerbates arm stress–related wear and tear, no matter how efficient the pitcher's delivery.6
Fatigue
Arm fatigue is perhaps one of the greatest risk factors associated with shoulder and elbow injuries.1,4,5 The shoulder provides an excellent example.
Large forces are placed on the shoulder during the act of pitching, specifically during the follow-through motion.7 The angular velocity of internal rotation ranges between 6000° and 7000° per second.8,9 At such high velocities, the shoulder girdle depends on more than a dozen muscles for its stability throughout the pitching motion. When these muscles become fatigued, their ability to provide the stability necessary for proper throwing mechanics declines in both the acceleration and deceleration phases.

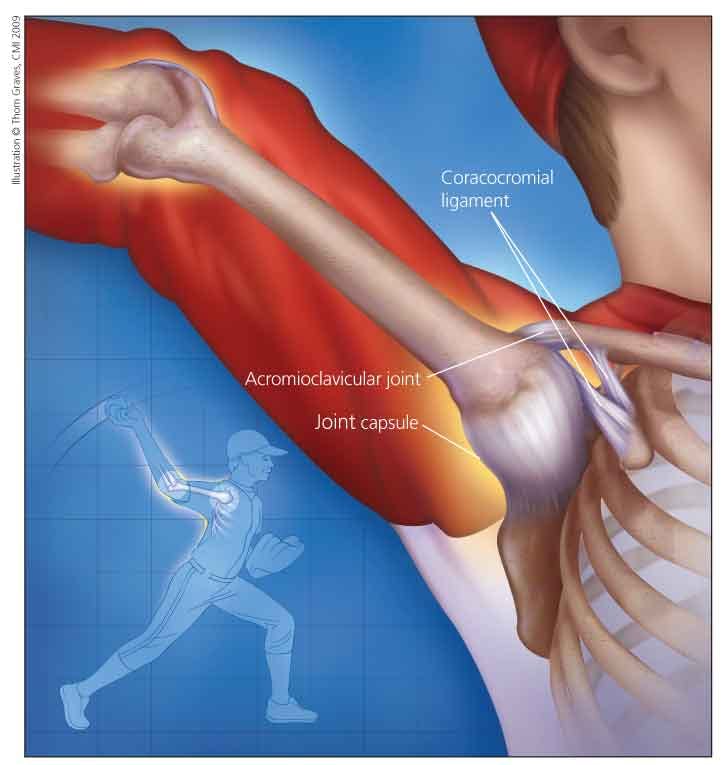
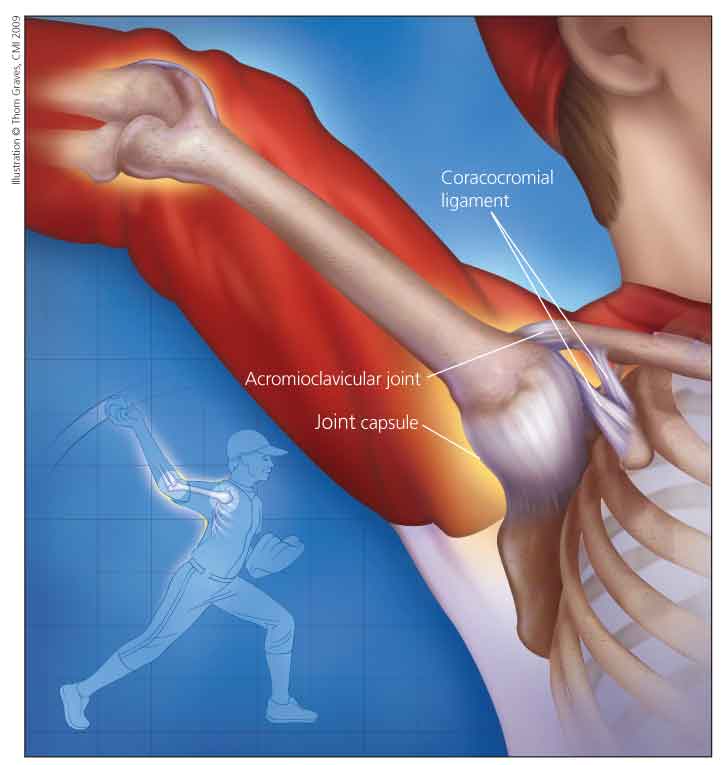
Figure 1 – "Dead arm syndrome" in a young pitcher is shown in this drawing. After ball release, the elbow is nearly extended, with the forearm pronated. The resultant force on the glenohumeral joint is distraction. The posterior shoulder musculature responds by providing a compressive force, but it may be too much for the musculature to resist fully. Therefore, the posteroinferior capsule is subjected to high tensile forces, resulting in hypertrophy over time. Pitchers with an internal rotation deficit typically respond to a stretching program when the deficit is detected at an early stage.
Failure of the scapular stabilizers to properly coordinate motion can result in damage to capsular and ligamentous elements in the shoulder. This sometimes is considered a "dead arm syndrome" (Figure 1) when a pitcher complains of decreased velocity, pain, and an inability to locate his or her pitches.10 This syndrome is thought to be the result of repeated microinstability over time; it results in sensory diminution and the aforementioned clinical scenario.
Pitch count
The factor most related to arm fatigue and overuse is the total number of pitches thrown, or pitch count, which has at least 3 important variations. The pitch count can be calculated by the number of pitches thrown per game, by the pitches thrown within any 1-week (7-day) period, and by the total pitches thrown throughout the course of a season.
Care should be taken to limit the amount of pitches thrown in a game, regardless of the pitcher's lack or level of complaints. Studies have shown that a high number of pitches thrown during a game is strongly associated with an increased incidence of arm injury.4,11 The risk of overuse injury also increases when the total number of pitches thrown in a given week or season exceeds safe limits.4,11 Guidelines have been established to reduce these risks and maximize safety by breaking down the maximum number of pitches that should be thrown by age-group per game, inning, and season.3,12,13
The number of pitches per inning is another aspect of pitch count that deserves consideration. A 45-pitch inning stresses the arm as much as a 75-pitch game at 15 pitches per inning.
Pitch type
The frequency of pitch type, or ratio of the various pitches a pitcher throws, also should be considered. Optimizing the ratio of fastballs to breaking balls and change-ups limits excessive exposure to a specific muscle group used for a given pitch; 60% to 65% fastballs, 20% to 25% breaking balls, and 15% to 20% change-ups has proved to be a benchmark of safety for pitchers of all ages.6
Research suggests that pitch type is not as strongly associated with an increased risk of injury as once thought. Older studies emphasized that the use of curveballs and other breaking pitches could lead to an increase in injury risk4,11; in particular, adolescents throwing curveballs had a 52% higher risk of arm pain and those throwing sliders were at 86% increased risk.
However, contradictory reports have shown that correctly throwing breaking pitches, particularly curveballs, is at least as safe as throwing fastballs.14,15 A recent study that measured rotational torques and forces experienced by the shoulder and elbow in pitchers found that throwing the fastball results in the highest values, followed by the curveball and then the change-up.14
At issue is difficulty in accurately measuring the technique used by young pitchers attempting to throw breaking balls. At the Little League level, poor technique abounds, and breaking balls are rarely thrown correctly, possibly leading to injury in the immature skeleton. Proper technique that does not result in excessive torque on the shoulder and elbow, but relies on proper grip and wrist position, may lead to the outcomes seen in recent motion analysis studies.6,14,15
It has been recommended that young pitchers limit pitch totals even more when they can throw at speeds in excess of 80 to 85 mph because tremendous forces are placed on the arm in acceleration and deceleration at these high velocities. In an immature arm, the stresses are just too great for joints, connective tissue, and bone.1,16,17
Lack of proper rest
Resting the throwing arm is the primary tool for combating overuse and fatigue. Rest allows muscles to return to a state of readiness after the onset of fatigue by replenishing proper chemical levels for muscle contraction, such as calcium ions and energy stores, and for minor injuries to heal.16
As is the case with pitch count limits, guidelines have been set that detail the amount of rest required after pitching in a game.3,13 Little League Inc mandates that players 16 years and younger who throw more than 61 pitches during the course of a game abstain from participating as a pitcher for 3 days. At higher levels of competition, pitchers who experience muscle failure because of high pitch totals require 2 to 3 days to recover. A recent study demonstrated a decreased passive range of motion in the shoulder and elbow of pitchers immediately after their outing that lasted more than 24 hours.18 These guidelines must take into account age, the number of pitches thrown in a game, mechanical efficiency, and functional strength to assess the appropriate length of recovery time that should be taken to ensure that pitchers' bodies are ready to participate safely in future games.6
Overparticipation
Participating in extra league play or activity with arm fatigue can increase the risk of injury.4,11 Young players should not play on more than 1 team during a season.13 If they do, pitching should be performed on only 1 of the teams.4
In locations where the weather permits, young baseball players playing year-round is not uncommon. Again, throwing year-round is acceptable, but pitching year-round is not. When the child pitches throughout the year, his arm lacks the ability to heal or completely recover from the constant barrage of stress and the repetitive microtrauma incurred on the mound throughout the course of a season. Pitchers are advised to abstain from high-intensity overhead activity, including pitching, for at least 3 months of the year.1,5,19
Another injury risk factor that has been suggested is skeletally immature pitchers performing weight lifting concurrently with pitching.4 Perhaps the problem is not with weight lifting but rather with the exercises chosen or misuse of the weight training program. The risk of injury may be reduced and performance improved with closed-chain bodywork for stability, mobility, and flexibility, as well as the use of light dumbbells, elastic cords, and plyoball training for joint integrity.

Figure 2 – This pyramid illustrates the levels of the authors' recommended fitness/rehabilitation program. Each level should be addressed thoroughly before an athlete progresses to the next level to avoid joint breakdown during pitching and other repetitive stress activities.
We advocate the use of a functional conditioning pyramid, which highlights these principles (Figure 2). Functional conditioning relies heavily on isometric muscle work and balancing the action of both agonists and antagonists.
Mechanistic considerations
A great deal of coordination and timing are required to generate the forces necessary for pitching. If during the act of throwing 1 event is mistimed or out of sequence, increased stress is placed on other areas of the body.20 For example, poor throwing mechanics associated with youth pitchers, and those fatiguing, are seen when trunk rotation occurs prematurely in the throwing motion and results in hyperextension (horizontal abduction) of the shoulder.19 This can lead to pathological mechanisms thought to be responsible for several entities, such as anterior laxity, internal impingement, labral lesions, and the dead arm syndrome. If a player learns proper mechanics early in his pitching career, this may help prevent arm and shoulder injuries as he advances to higher levels of play.21
The primary culprit in the dead arm syndrome is the tight posteroinferior (PI) shoulder capsule (see Figure 1). The PI capsule is hypothesized to become hypertrophied in the follow-through tensile motion of throwing.10 After ball release, the elbow is nearly extended, with the forearm pronated. The resultant force on the glenohumeral joint is one of distraction. Such a force can reach up to 750 N.22 The posterior shoulder musculature responds by providing a compressive force (decelerating). However, such a force may be too much for the musculature to resist fully, especially when it is fatigued. Therefore, the PI capsule is subjected to high tensile forces, resulting in hypertrophy over time.
Pitchers who have a tight PI capsule present with decreased internal rotation in their pitching arm compared with the contralateral side. This presentation should be considered a red flag, indicating a "shoulder at risk." Pitchers with an internal rotation deficit typically respond to a stretching program and isometric shoulder and scapular strengthening that emphasizes the posterior structures (decelerators).
Sports medicine has identified the pathology that results from poor mechanics. However, coaches need to reject the conventional wisdom about pitching mechanics and to understand and embrace science-based motion analysis for their information and instruction protocols.
FUNCTIONAL CONDITIONING NEEDED
Proper conditioning is vital to the health and longevity of the throwing arm,16,20,23 and functional strength, endurance, and flexibility are important aspects of conditioning. Achieving balanced strength in the many muscles involved in the act of throwing prevents any 1 muscle from becoming fatigued or overloaded.5
Muscle imbalance, in this case in a pitcher demonstrating overload and fatigue, can manifest as SICK (Scapular malposition, Inferior medial border prominence [scapular], Coracoid pain and malposition, and scapular dysKinesis) scapula syndrome. This syndrome is managed with a program of scapular strengthening and stabilization.
Overall, a balanced and preventive program of physical strengthening and conditioning can delay the onset of fatigue and help young pitchers maintain healthy function. Such a program can be addressed during the off-season when the athlete is not throwing the baseball, and healthy habits can be carried forward into the next season.
CONCLUSION
Knowledge about throwing injuries should be used to minimize and prevent them. Guidelines for injury prevention have a common unifying theme: limit the number of high-intensity pitches the young arm is exposed to and allow ample time for arm rest in the days after a performance. Many youth leagues have instituted maximums for the number of pitches a pitcher is allowed to throw in a given game or a given week. Coaches, parents, and players need to keep track of these totals.
Refraining from throwing at full strength for selected periods after pitching in a game gives the arm the necessary time to regain strength and repair minor damage. Developing proper mechanics and performing conditioning exercises are proactive measures a young pitcher can use to minimize the risk of sustaining an injury to the throwing arm while pitching. A physician's recognition of the pattern of injury and examination signs of a player who is "breaking down" helps prevent irreversible structural damage. League officials, coaches, parents, and players should be kept informed of new information relating to the safety of young players as it becomes available. Early recognition combined with rest and a supervised rehabilitation program is likely to result in rapid, healthy return to play.
References:
References1. Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med. 2004;32:1158-1164.
2. About USA Baseball. USA Baseball. 2007. http://web.usabaseball.com/about/. Accessed February 18, 2009.
3. Little League Online. Baseball & Softball. Little League Implements New Rule to Protect Pitchers' Arms. 2006. www.littleleague.org/media/newsarchive/03_2006/06pitch_count_08-25-06.htm. Accessed February 18, 2009.
4. Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33:1803-1810.
5. Olsen SJ 2nd, Fleisig GS, Dun S, et al. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905-912.
6. House T, Thorburn D. Arm Action, Arm Path, and the Perfect Pitch: Building a Million-Dollar Arm. 2009. Coaches Choice. www.coacheschoice.com. Accessed February 19, 2009.
7. Werner SL, Gill TJ, Murray TA, et al. Relationships between throwing mechanics and shoulder distraction in professional baseball pitchers. Am J Sports Med. 2001;29:354-358.
8. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther. 1993;18:402-408.
9. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233-239.
10. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology, part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404-420.
11. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463-468.
12. Andrews JR, Fleisig G. How many pitches should I allow my child to throw? USA Baseball News. 1996. www.youcanbefit.com/Pitches.pdf. Accessed February 18, 2009.
13. Little League Online. Baseball & Softball. Little League Refines Baseball Pitching Rules for 2008. 2007. www.littleleague.org/media/newsarchive/2007stories/07pitching_rule_reg_changes_10_07.htm. Accessed February 18, 2009.
14. Dun S, Loftice J, Fleisig GS, et al. A biomechanical comparison of youth baseball pitches: is the curveball potentially harmful? Am J Sports Med. 2008;36:686-692.
15. Fleisig GS, Kingsley DS, Loftice JW, et al. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am J Sports Med. 2006;34:423-430.
16. Benjamin HJ, Briner WW Jr. Little league elbow. Clin J Sport Med. 2005;15:37-40.
17. Magra M, Caine D, Maffulli N. A review of epidemiology of paediatric elbow injuries in sports. Sports Med. 2007;37:717-735.
18. Reinold MM, Wilk KE, Macrina LC, et al. Changes in shoulder and elbow passive range of motion after pitching in professional baseball players. Am J Sports Med. 2008;36:523-527.
19. Keeley DW, Hackett T, Keirns M, et al. A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop. 2008;28:452-459.
20. Limpisvasti O, ElAttrache NS, Jobe FW. Understanding shoulder and elbow injuries in baseball. J Am Acad Orthop Surg. 2007;15:139-147.
21. Andrews JR, Fleisig GS. Preventing throwing injuries. J Orthop Sports Phys Ther. 1998;27:187-188.
22. Levitz CL, Dugas J, Andrews JR. The use of arthroscopic thermal capsulorrhaphy to treat internal impingement in baseball players. Arthroscopy. 2001;17:573-577.
23. Whiteley R. Baseball throwing mechanics as they relate to pathology and performance-a review. J Sports Sci Med. 2004;6:1-20.
Â











 May Offer Over PPIs, with Adelina Hung, MD")



