ACR/AAHKS Introduces Guidelines for Optimal Timing of Knee and Hip Arthroplasty
The guidelines were created using a panel of rheumatologists, orthopedic surgeons, and patients.
The American College of Rheumatology (ACR) and the American Association of Hip and Knee Surgeons (AAHKS) released a summary of its new guidelines for patients with symptomatic, radiographic, moderate-to-severe osteoarthritis (OA) and osteonecrosis (ON) of the hip and knee who have failed nonoperative therapy. The guidelines focused on the timing of elective hip and knee arthroplasty (TJA) or delays for medical optimization for this patient population.


“For patients with symptomatic moderate to severe osteoarthritis or osteonecrosis of the hip or knee who have been indicated for total hip or total knee arthroplasty, the efficacy of additional nonoperative treatments, such as physical therapy, anti-inflammatories, and injections is unknown,” stated Charles P Hannon, MD, MBA, Assistant Professor of Orthopedic Surgery at Washington University in St. Louis and co-literature review leader of the guideline. “In addition, for patients with certain risk factors, such as obesity, which are linked to increased risk and poorer outcomes, the benefit of delaying surgery to modify these risk factors is not well established. For these reasons, a guideline needed to be created.”
The guidelines were created using a panel of rheumatologists, orthopedic surgeons, and patients. The Patient Panel underlined the importance of shared decision-making between patients and clinicians. A systematic literature review was conducted to identify the clinically relevant population, intervention, comparator, and outcomes (PICO) questions. Consensus was reached by taking evidence, patient preferences, and clinical expertise into consideration.
“This shared decision-making process should comprehensively discuss the unique risks and benefits of the procedure for the individual patient,” said Susan M. Goodman, MD, attending rheumatologist at the Hospital for Special Surgery and co-principal investigator of the guideline. “Patients with medical or surgical risk factors as described in this guideline should be counseled as to their increased risks, and preoperative attempts to modify these risk factors through efforts such as weight loss, glycemic control, or smoking cessation should be encouraged.”
Although all recommendations were deemed conditional, a high consensus for all recommendations was established. Evidence for the recommendations was categorized as low or very low quality, due in part to indirectness.
Highlights
The following recommendations are for patients with radiographically moderate-to-severe OA or ON of the hip or knee and moderate-to-severe pain or loss of function who have been indicated for elective TJA and have completed at least 1trial of nonoperative therapy.
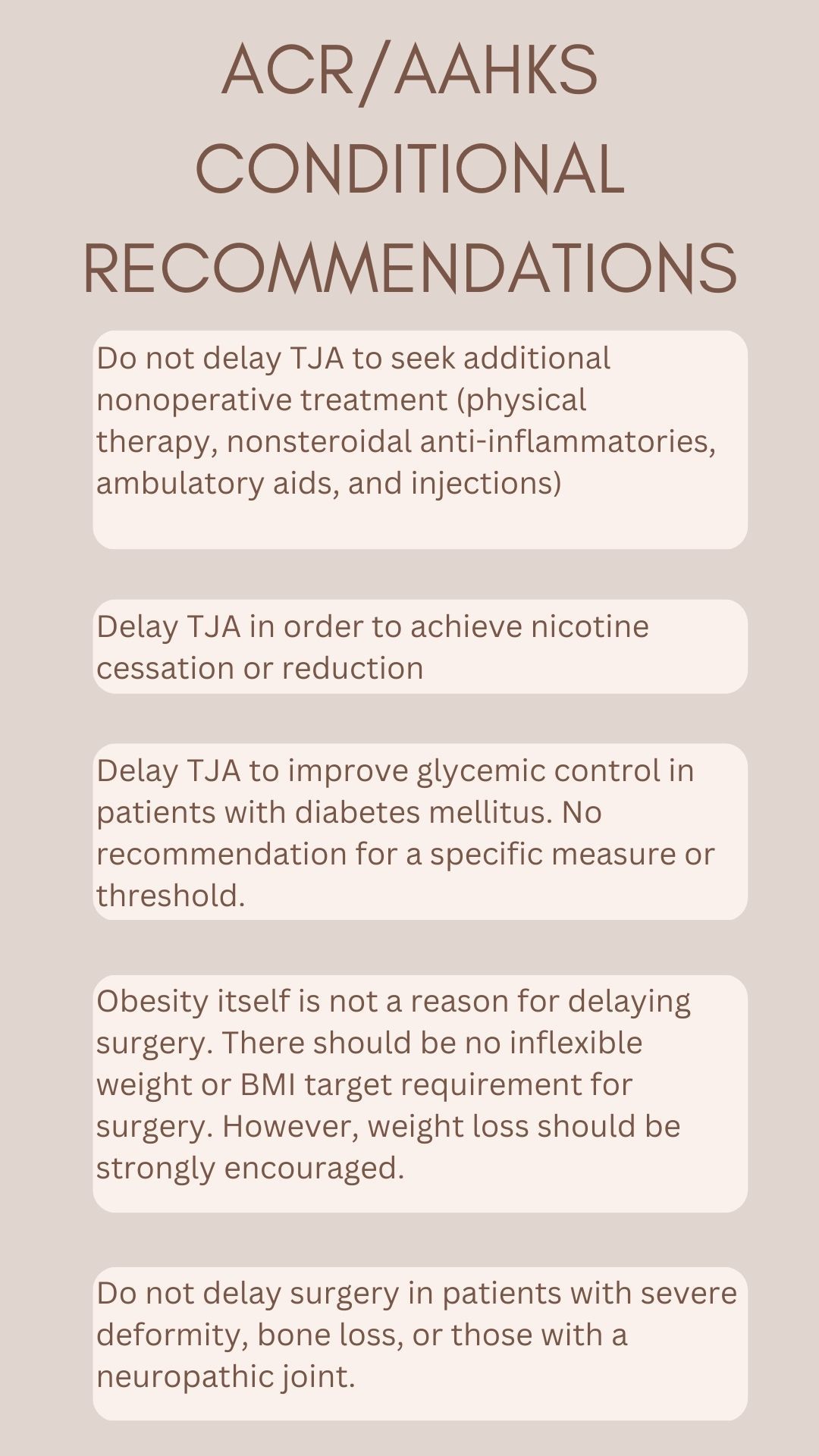
- It is conditionally recommended to proceed to TJA without delay over delaying arthroplasty 3 months
- It is conditionally recommended to proceed to TJA without delay over delaying arthroplasty for a trial of physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDS), braces and/or ambulatory aids, intra-articular glucocorticoid injections, or viscosupplementation injections.
- For patients with a body mass index (BMI) >50, it is conditionally recommended to proceed to surgery without delay to achieve a BMI of <50.
- For patients with a BMI of 40 – 49, it is conditionally recommended to proceed to surgery without delay to achieve a BMI of <40.
- For patients with a BMI of 35 – 39, it is conditionally recommended to proceed to surgery without delay to achieve a BMI of <35.
- It is conditionally recommended that patients with poorly controlled diabetes mellitus delay TJA to improve glycemic control.
- It is conditionally recommended that patients with nicotine dependence delay arthroplasty for nicotine use reduction/cessation.
- It is conditionally recommended that patients with bone loss with deformity or severe ligamentous instability proceed to TJA without delay over delaying arthroplasty for optimization of non-life-threatening conditions.
- It is conditionally recommended that patients with a neuropathic joint proceed to TJA without delay over delaying for optimization of non-life-threatening conditions.
A full manuscript of the guideline is expected to be jointly published in ACR and AAHKS journals in 2023.









 May Offer Over PPIs, with Adelina Hung, MD")





